Article Text

Abstract
Objectives HIV point-of-care testing (POCT) has been available in Manitoba since 2008. This study evaluated the effectiveness of POCT at identifying individuals with previously unknown HIV status, its effects on clinical outcomes and the characteristics of the populations reached.
Methods A retrospective database review was conducted for individuals who received HIV POCT from 2011 to 2014. Time to linkage to care and viral load suppression were compared between individuals who tested positive for HIV using POCT and controls identified as positive through standard screening. Testing outcomes for labouring women with undocumented HIV status accessing POCT during labour were also assessed.
Results 3204 individuals received POCT (1055 females (32.9%) and 2149 males (67.1%)), being the first recorded HIV test for 2205 (68.8%). Males were more likely to be targeted with POCT as their first recorded HIV test (adjusted OR (AOR) 1.40). Between the two main test sites (Main Street Project (MSP) and Nine Circles Community Health Centre), MSP tested relatively fewer males (AOR 0.79) but a higher proportion of members of all age groups over 30 years old (AOR 1.83, 2.51 and 3.64 for age groups 30–39, 40–49 and >50, respectively). There was no difference in time to linkage to care (p=0.345) or viral load suppression (p=0.405) between the POCT and standard screening cohorts. Of 215 women presenting in labour with unknown HIV status, one was identified as HIV positive.
Conclusions POCT in Manitoba has been successful at identifying individuals with previously unknown HIV-positive status. Demographic differences between the two main testing sites support that this intervention is reaching unique populations. Given that we observed no significant difference in time to clinical outcomes, it is reasonable to continue using POCT as a targeted intervention.
MeSH terms HIV infection; rapid HIV testing; vertical infectious disease transmission; community outreach; service delivery; marginalised populations.
- HIV testing
- screening
- service delivery
- outreach services
- antenatal HIV
Statistics from Altmetric.com
Background
An estimated 21% of HIV-positive individuals in Canada remain undiagnosed.1 Despite the interventions that can be made once HIV-positive status is established, about two-thirds of Canadians have never received HIV testing.2 Fear of positive status and risk underappreciation have been identified as factors contributing to individuals remaining untested.3 4 Among minority groups, marginalisation and complicated relationships with the healthcare system present additional barriers to testing.5 6 Certain groups considered to be at increased risk of infection—men who have sex with men and people who use drugs—tend to have higher rates of testing; however, other at-risk groups, such as Indigenous peoples and recent immigrants, remain disproportionately undertested.2 5 Thus, targeted testing strategies are needed to discern previously unidentified HIV status.
The INSTI HIV-1/HIV-2 Rapid Antibody Test (bioLytical Laboratories) was approved by Health Canada for the presumptive diagnosis of HIV infection in 2005.7 The single-use point-of-care testing (POCT) detects HIV antibodies in a small blood sample obtained from a patient’s finger. Performance characteristics are considered equivalent in sensitivity and specificity to the standard method of HIV screening, which is enzyme immunoassay (EIA).8 9 Results are delivered within minutes of testing. A negative (‘non-reactive’) POCT is considered definitive (except in the window period), giving patients peace of mind and an opportunity for preventative interventions in a single encounter.7 In Canada, while presumptive diagnoses from positive (‘reactive’) POCT must be serologically confirmed, linkage to care can begin immediately following POCT.
Thanks to its portability and acceptability, POCT lends itself to non-traditional settings.10 POCT has successfully identified undiagnosed HIV infection in individuals in various outreach settings.11 12 Since 2001, the US Centers for Disease Control has recommended rapid HIV testing during labour for women with limited prenatal care (PNC) and/or unknown HIV status, as the risk of vertical transmission can be reduced from 25%–40% to under 5% with intrapartum antiretroviral treatment (ART).13
POCT has been available in Manitoba since 2008, with the aim of increasing HIV screening among marginalised populations. To date, there has been no assessment of the populations accessing POCT in Manitoba. The use of POCT in accessing previously untested individuals has also not been analysed. The goal of this study was to begin a critical evaluation of POCT in Manitoba and contribute to the growing body of evidence supporting POCT implementation.
Methods
The following is presented using the SQUIRE 2.0 Framework.14 This study had three outcomes of interest; these have been divided into individual sections.
Context
Following its successful introduction to Nine Circles Community Health Centre (NCCHC) in 2008,15 additional POCT sites were selected based on their suitability to the goal of POCT implementation in Manitoba: increasing the identification of HIV-positive individuals from marginalised communities.16 These sites include Winnipeg’s Main Street Project (MSP) and the obstetrical triages in Winnipeg’s Women’s Hospital.
All non-POCT HIV testing—including screening, confirmatory testing and ongoing analyses—in Manitoba is performed at Cadham Provincial Laboratory (CPL), and all sites that offer HIV POCT send monthly reports to CPL. Thus, a discrete, centralised and complete dataset was available for analysis.
Interventions
We conducted a critical evaluation of certain aspects of the POCT initiative in Manitoba. Analyses consisted of retrospective chart reviews of HIV testing records available to CPL. Demographic information obtained included date of birth, gender, initials and Personal Health Information Number (PHIN). Clinical data obtained from the database included the date, site and result of initial HIV screening, as well as the date and method of subsequent HIV testing, including viral load (VL) testing when applicable. Testing practices at the sites analysed are as follows:
NCCHC operates a weekly drop-in STBBI testing clinic. POCTs are available to clients during clinic times and during privately arranged STBBI testing and counselling appointments. Site records did not specify under which circumstance POCTs were performed.
MSP is the site of Winnipeg’s Intoxicated Persons Detainee Area (IPDA) and sees a large volume of marginalised and high-risk clients. On discharge from IPDA, clients are offered POCT by the paramedic on service. Clients with reactive tests are provided transportation or referral to NCCHC for confirmatory testing, depending on NCCHC clinic hours. Site records from MSP did not indicate the disposition of clients following receipt of POCT results.
Women presenting to the Labour and Delivery Unit (LDU) of Women’s Hospital in active labour, with undocumented HIV status during her current pregnancy, were eligible to be offered POCT. ‘Undocumented HIV status’ included a prenatal record without a completed HIV test or lack of a prenatal record on presentation to the LDU. Nurses were instructed to offer testing to eligible women while performing their standard admission assessments at obstetrical triage.
The INSTI HIV-1/HIV-2 Rapid Antibody Test was used for all POCT administered in this study.
Ethical considerations
This study received approval from the University of Manitoba’s Health Research Ethics Board (HREB Approval: H2015104) and the Province of Manitoba’s Health Information Privacy Committee.
Client and site demographics
We compared the demographics of clients accessing POCT at the two main testing sites in Winnipeg, NCCHC and MSP. Our aim was to assess whether previously untested individuals were being tested and whether the two sites accessed different populations.
Study of the intervention
HIV testing records for individuals who received HIV POCT between 1 April 2011 and 31 December 2014 were reviewed. Initial data manipulation included removing out-of-province PHINs and individuals with incomplete demographic data. Six individuals who identified as transgender were excluded from our analysis, as the small number of people in this group precluded analysis as a separate group. A total of 3204 charts were included in our analysis. Client demographic information was used to assess age and sex characteristics of the population accessing POCT in Manitoba.
Regression analyses were undertaken to identify demographic differences between previously untested individuals and those who had received previous HIV testing. Unique individuals who received POCT over the study period were divided into the two groups based on their HIV testing history as available through CPL records. Then, associations between patient demographics and the site where individuals received their first POCT were analysed by dividing all individuals into two new groups based on this site.
Measures
The proportion of previously untested individuals among all persons who received HIV POCT was determined by reviewing testing histories among all individuals who received POCT and evaluating for a record of HIV testing prior to first POCT. Corresponding EIA data that were linked to the POCT data extended from 29 August 2009 (the earliest EIA date in the dataset) to 31 December 2014. There was no record kept of the number of refusals.
Analysis
Logistic regression was used to assess associations between the above outcome and predictor variables. Bivariate analyses were first completed, and all variables with p values of 0.1 or less were considered for inclusion in multivariable analyses. The effect of removing individual predictor variables was assessed by the likelihood ratio test. All statistical analysis was done with Stata (V.11). A p value of <0.05 was considered statistically significant.
Clinical outcomes
We evaluated the difference in time to clinical outcome measures available to us (linkage to care and VL suppression) between individuals identified as HIV positive through POCT versus EIA. These analyses were based on patients with reactive POCT from NCCHC and MSP (n=23) that were compared with control sample populations with positive EIA at NCCHC, Bridgecare Clinic and Klinic from 1 January 2010 and 1 June 2015 (n=100). Bridgecare Clinic and Klinic were felt to be appropriate controls, as similar to NCCHC, they serve large inner-city, sexual and gender minority and newcomer populations.
Study of the intervention
Screened new positives in each group (POCT vs EIA) were analysed for the proportion that achieved the outcome of interest. Time to linkage to care was defined by the proxy measure of the date of first recorded VL testing. Time to VL suppression was defined by the proxy measure of the date of first recorded undetectable VL. Data were collected from both groups from the time of reactive/positive screening test until achieving the outcome of interest or the end of the study period. Any patient who was newly diagnosed with HIV following a screening test was eligible for inclusion.
Measures
A number of patients (n=14; 10 males and 4 females) in the EIA group were found to have undetectable HIV VL at the time of initial analysis. These individuals may represent pretreated newcomers to Manitoba presenting for an initial health evaluation or HIV elite controllers. These patients were included in our time to linkage to care analysis but not our time to VL suppression analysis.
Analysis
Wilcoxon analysis of survival to clinical outcome was used to assess statistical significance of the mean time to clinical outcomes between the two groups. Univariate descriptive statistical analysis was conducted using a non-parametric procedure, Kaplan-Meier Method, to estimate overall survival. All data were analysed using SAS (V9.4). A p value of <0.05 was considered statistically significant.
Obstetrical triage
Study of the intervention
The POCT site records from the Women’s Hospital LDU were reviewed for reactive tests out of the 215 total POCTs administered. Follow-up HIV testing data for children born to HIV-positive women identified by POCT at time of delivery was available through CPL’s records.
Measures
Records regarding the number of eligible women who refused testing during labour were not kept. Demographic and delivery data were collected by the LDU but was not available to members of the study team. LDU documentation available to the study team did not indicate whether tested women received PNC; therefore, this could not be used to stratify our analyses.
Analysis
LDU site records were reviewed for positive POCT screens. Qualitative reports of neonatal follow-up for the exposed infant were reviewed.
Results
Client and site demographics
Of the 3204 individuals who received POCT during the study period, 2205 (68.8%) had no previously recorded HIV test. Of the 3204 individuals who received POCT during the study period, 1073 did not have a PHIN recorded. These non-PHIN individuals were matched to testing histories using a combination of first and last initials, date of birth and gender. Due to the potential uncertainty that this matching process introduced, secondary analyses were performed using only data from individuals who could be identified by PHIN; however, these secondary analyses did not change the results compared with the whole data set and are therefore not included.
Table 1 shows demographic differences for individuals accessing their first HIV screening test through POCT versus EIA. Males were significantly more likely to receive POCT as their first screening test. In bivariate analysis, individuals aged 50 years and older were more likely to receive POCT as their first screening test; however, in multivariate analysis only the relationship with gender remained significant.
Demographic characteristics of individuals who received HIV POCT over the study period (n=3204) and multivariable analysis of differences between those whose first test was POCT and those who had received EIA prior to an initial POCT
To identify associations between the place where an individual received their first POCT and patient demographics, logistic regression was conducted using location (NCCHC vs MSP) as the outcome variable for the complete dataset of 3204 people. Adjusted ORs are shown in table 2. In our situation, females were more likely to be tested at MSP, as were all age groups over the age of 30 years.
Demographic characteristics of individuals accessing a first HIV POCT at the two main testing sites offering HIV POCT in Manitoba (n=3204) and multivariable analysis of differences
Review of frequency analysis of all POCT administered at NCCHC and MSP during the study period demonstrated a rapid increase in testing at MSP in 2014, without a clear corresponding drop-off at NCCHC.
Clinical outcomes
The majority of screened new positives in the POCT and EIA cohorts were male (56.5% and 63%, respectively). Overall, 101 (82.1%) of the 123 newly identified HIV-positive individuals were successfully linked to care. Of the 87 individuals linked to care who did not initially have undetectable VLs, 36 (33.3%) achieved VL suppression by the end of the study period. Males and females showed no clear differences by test type for these two clinical outcomes, therefore gender-specific data are not shown. Stratification by test type showed no difference between POCT and EIA for linkage to care; however, achievement of undetectable VL was 63.2% for individuals identified by POCT versus 29.3% for all individuals identified by EIA and linked to care and 35.2% of EIA without initially undetectable VLs (table 3).
Number and proportion of new HIV positives (n=122) stratified by test type who were linked to care and, of those linked to care, achieved viral load suppression
With the data available, analyses of survival to clinical outcome are shown in figure 1. There was no statistically significant difference in time to either clinical outcome between the POCT and EIA groups (p=0.3449 for time to linkage to care and p=0.4046 for time to VL suppression, respectively).
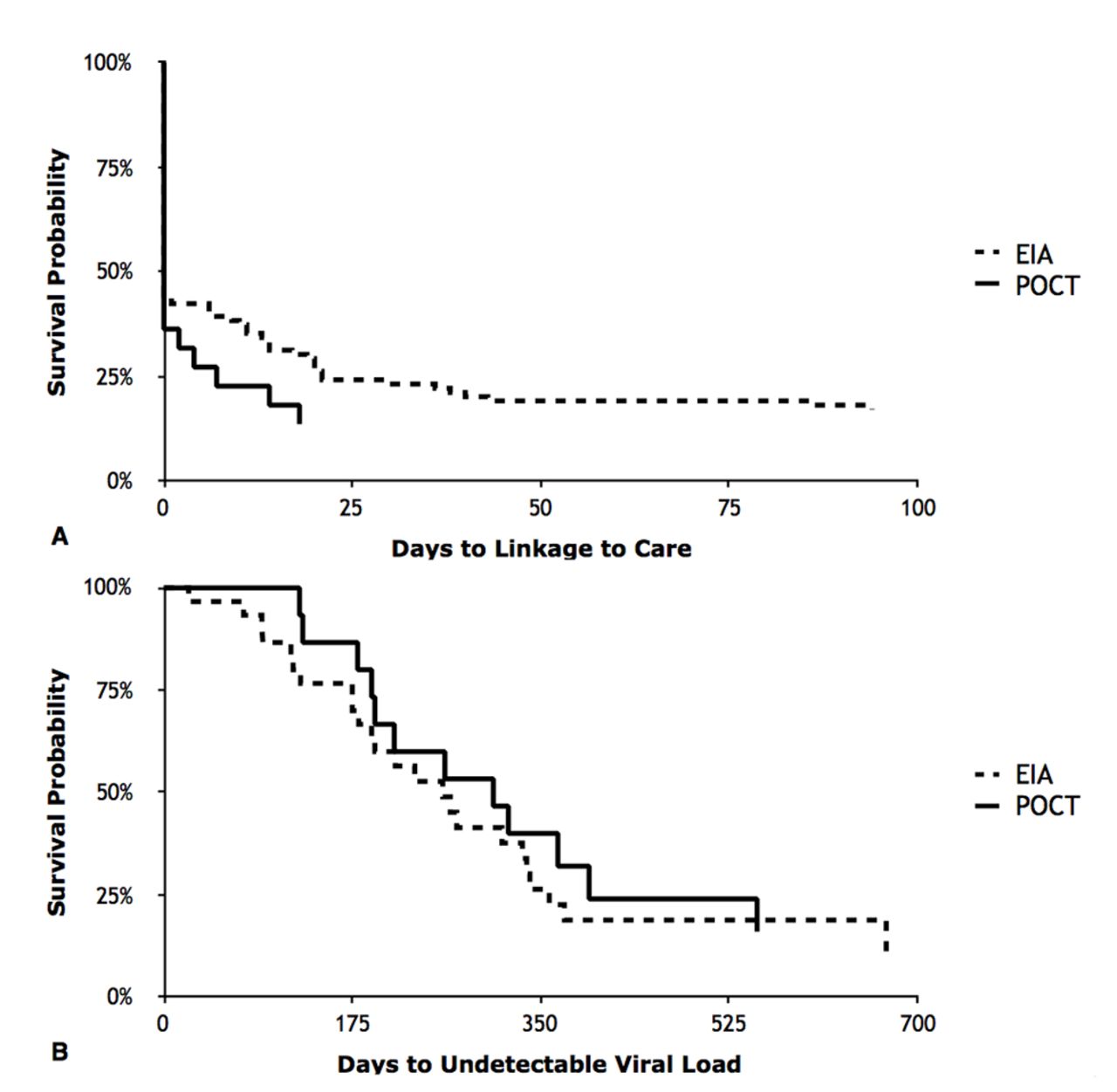
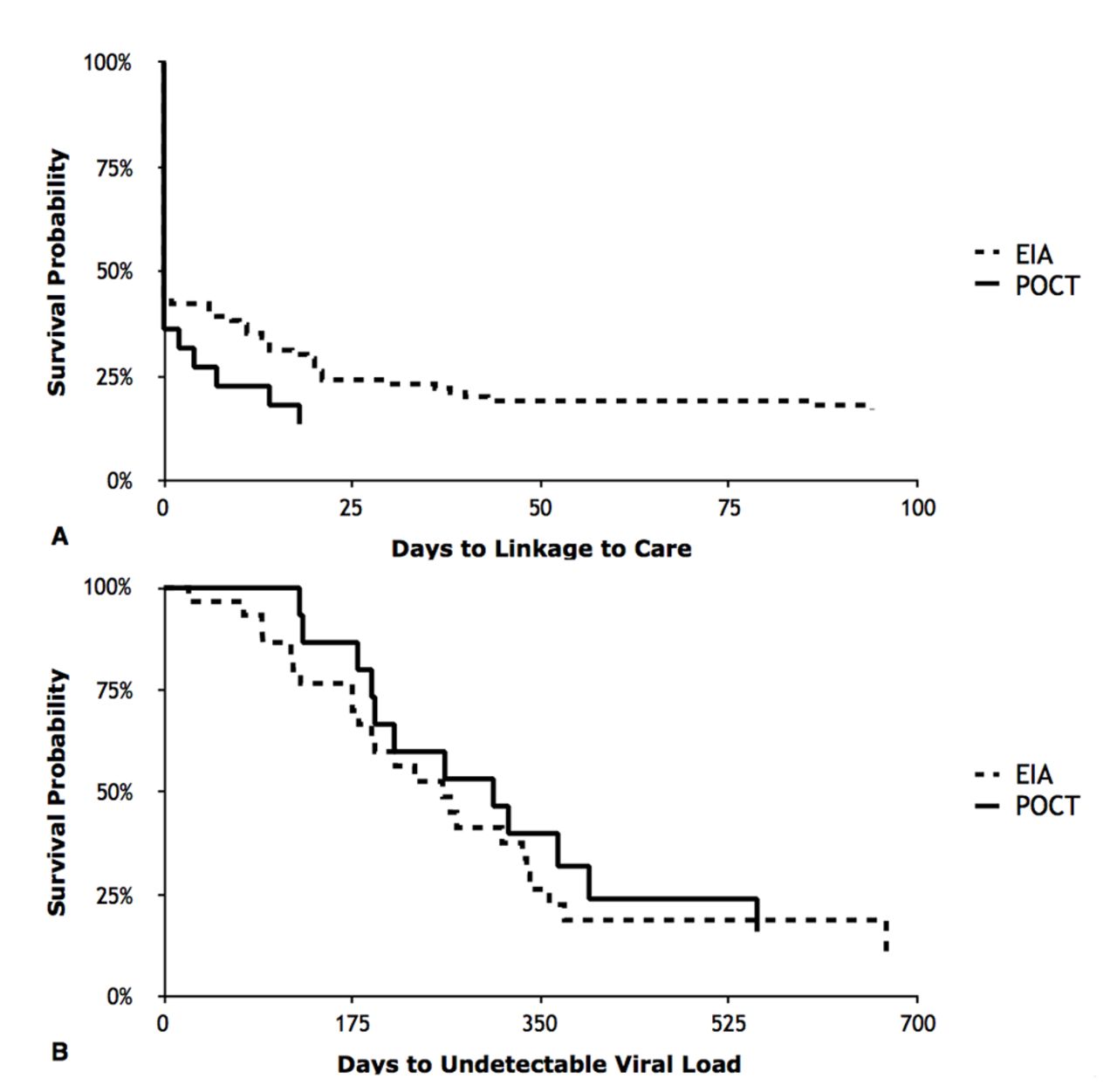{kind=link}
Survival analyses comparing clinical outcomes between individuals identified as HIV positive via point-of-care testing (POCT) or by standard serological methods (EIA) for (A) time to linkage to care (p=0.3449) and (B) time to viral load suppression (p=0.4046). EIA, enzyme immunoassay.
Obstetrical triage
Of the 215 women presenting to the Women’s Hospital in active labour with unknown HIV status, one (0.46%) was newly identified as HIV positive through POCT. ART was initiated in labour, and following HIV PCR follow-up, the infant was identified as HIV negative.
A full cost-effectiveness analysis was not completed. However, assuming a 25% vertical transmission rate for untreated HIV, the number needed to screen to prevent one case of congenital HIV in this study would be 860.
Discussion
POCT in Manitoba has been able to reach previously untested individuals. The majority of clients who accessed POCT during our study period (68.8%) had no recorded HIV test prior to their initial POCT. We observed that men were more likely to have their first recorded HIV test be POCT. We observed demographic differences between the populations accessing POCT at the two main testing sites in Winnipeg. We did not observe a significant difference in the time to linkage to care or time to VL suppression between individuals identified as HIV positive by POCT versus by EIA. One (0.46%) out of 215 labouring women screened for HIV using POCT was identified as HIV positive.
Our study had important limitations. Our analyses were retrospective chart reviews, thus, data were non-random. Demographic data were limited to age and gender and did not allow for statistical corrections to be made for additional risk factors that might contribute to poorer health outcomes. We did not stratify our analysis of first POCT site demographics into those who had received previous HIV testing and those who had not.
Using the date of first recorded VL as a proxy for linkage to care may not have been a perfect reflection of the individual’s first contact with their HIV care team. However, in the absence of a formal first clinic appointment date, we chose to use the date of first VL, given that the Manitoba HIV Program confirmed that individuals would typically have VL blood work performed at their first visit.
For our analysis of time to VL suppression, we could not determine whether every patient who was retained and receiving regular VL testing was on ART from the date of their initial VL. In keeping with contemporary guidelines,17 we assumed everyone returning for regular VL was on ART. We did not correct our analyses of VL suppression for the ART initiation guidelines that would have been in place at the time of each individual’s treatment. We did not impose a strict time measure on when we would assess for the achievement of clinical outcomes, rather keeping the end point open until the end of the study period.
Our study database was limited to data from 2009 onwards; therefore, it is conceivable that some of the individuals with no record of HIV testing prior to receiving POCT may have received testing prior to 2009. However, this likely represents only a small proportion of the total number of people who had no HIV test recorded prior to receiving their initial POCT.
A major strength of our study is that we have been able to demonstrate the complementary effect of multiple testing sites, with different approaches to testing clients. The differing approaches to testing at NCCHC and MSP accessed demographically different populations. The successes at MSP would seem to speak to the value of introducing POCT to settings that are not traditionally ‘medical’, particularly if we hope to reach populations that have barriers to accessing healthcare.
Our sample sizes were small; however, we believe that our analysis of clinical outcomes demonstrates that POCT is not an inferior means of identifying HIV-positive individuals with respect to clinical outcomes. We believe this lends itself to further application of POCT in appropriate settings. Unfortunately, proportions of individuals linked to care and achieving VL suppression remain less than 100%, reinforcing that further work must be done to retain individuals in HIV care, no matter how they are identified.
In Winnipeg’s inner city, rates of inadequate PNC are as high as 21.5%.18 Many of these women, which include large Indigenous and newcomer cohorts, would also be considered at high risk for HIV. Consistent with other recent studies,19 20 POCT appears to be an effective means of identifying previously unknown HIV status in labouring women and informs rapid decision making for initiation of ART during labour.20 ,21 Identifying women in this way provides an avenue for interventions into their personal health and the health of future pregnancies, as well as for identifying infants at high risk for neonatal HIV infection. Our intervention was easily incorporated into the standard obstetrical triage assessment performed in our LDU. Operational costs were essentially limited to the cost of the screening test itself, roughly $C16, as well as the cost of confirmatory testing and intrapartum ART for screened new positives. Recognising that inadequate PNC and unknown HIV infection in pregnancy is prevalent in the developed world,18 19 we believe that our study strengthens the emerging evidence supporting POCT in labour.
The data presented here suggest that POCT in Manitoba has been able to reach previously untested individuals and identify individuals with previously unknown HIV-positive status. Our analyses have been conducted on an emerging dataset. With continued analysis, we believe that we will see further evidence supporting the use of POCT. Additional areas for analysis include assessment of STI testing behaviours before and after receiving HIV POCT, examining for differences in rates of retention in care between individuals identified by POCT versus EIA and more thorough demographic analysis and stratification, which will help to determine who remains excluded from healthcare and HIV testing.
Key messages
Implementing point-of-care testing (POCT) as a structured intervention in diverse settings can lead to previously untested individuals receiving HIV testing and identification of individuals with previously unknown HIV-positive status.
Clinical outcomes do not appear to be significantly different between individuals identified as HIV positive by POCT versus enzyme immunoassay.
HIV POCT in obstetrical triage can be used to identify women with unknown HIV status and inform treatment decisions and follow-up for mother and infant.
Acknowledgments
This study was conducted as part of the University of Manitoba’s Med II Summer Research Program and received funding from the University of Manitoba. The findings described in this study were presented at the AMMI-CACMID Annual Conference 2016 in Vancouver, BC, Canada. Attendance at the AMMI-CACMID conference was supported by the Alan Klass Memorial Program for Health Equity. The authors of this study would like to acknowledge the contributions of Roy Cole and Stella Leung to this project. Roy Cole was responsible for the creation of the study databases, using information available to Cadham Provincial Lab. Stella Leung performed Wilcoxon and Kaplan-Meier analysis on time to linkage to care and time to viral load suppression data. The study would not have been possible without the support of the staff at Cadham Provincial Lab. The authors would also like to acknowledge the support of Nine Circles Community Health Centre, the Main Street Project and WRHA’s Street Connections Program.
Footnotes
Handling editor Jackie A Cassell
Contributors JBJ was responsible for the chart review, data extraction, data collation, basic data analysis, writing and preparing the manuscript and formatting the tables and figure. JLW was responsible for statistical analysis of demographic data and contributed to the methods section. JB provided background information and access to HIV testing records and POCT site records through his capacities as associate medical director of CPL and his involvement in the HIV POCT Program in Manitoba. JB and JJNR were responsible for the original idea for this research project. All authors provided edits to the draft manuscript, and read and approved the final manuscript. Roy Cole was responsible for the creation of the study databases, using information available to Cadham Provincial Lab. Stella Leung performed Wilcoxon and Kaplan-Meier analysis on time to linkage to care and time to viral load suppression data.
Competing interests None declared.
Ethics approval University of Manitoba Bannatyne Campus Research Ethics Board (HREB Approval: H2015104).
Provenance and peer review Not commissioned; externally peer reviewed.