Article Text

Abstract
Objectives HIV testing is an important step towards diminishing incident infections. Rapid self-tests whose use is becoming more common in France could help increase access to testing, yet could fail to diagnose HIV during acute HIV infection (AHI). The aim of the present study was to evaluate HIV-detection sensitivity of a commonly used rapid self-test (STAT-VIEW HIV1/2), compared with another point-of-care rapid test (INSTI), among patients presenting with AHI.
Methods Individuals tested at Saint-Antoine Hospital (Paris, France) with negative or indeterminate western blot (WB) results and detectable HIV-RNA were included. Rapid tests were performed retrospectively on stored serum. Patients with and without reactive rapid tests were compared, while probability of having a reactive test was modelled across infection duration using logistic regression.
Results Of the 40 patients with AHI, 23 (57.5%) had a reactive STAT-VIEW rapid test. Patients with non-reactive versus reactive tests had a significantly shorter median time since infection (p=0.01), time since onset of symptoms (p=0.009), higher proportion with Fiebig stage III versus IV (p=0.003), negative WB results (p=0.007), higher HIV-RNA levels (p=0.001) and lower CD4+ and CD8+ cell count (p=0.03, p<0.001, respectively). When examining sensitivity over the course of AHI duration, the probability of HIV detection was 75.5% at 5 weeks from HIV transmission. The INSTI provided similar results with respect to proportion of reactive tests (62.5%), determinants for non-reactive test and probability of HIV detection at 5 weeks of infection (85.0%).
Conclusions Over half of AHI patients had reactive serology using the STAT-VIEW rapid self-test when performed on serum samples. Considering that detection sensitivity increased substantially over infection time, individuals should not rely on a negative result to accurately exclude HIV infection within at least 5 weeks of potential HIV exposure. Notwithstanding strong recommendations against rapid test use during AHI, some utility in detecting HIV is observed 5–12 weeks after transmission.
- HIV
- HIV primary infection
- HIV testing
- Point-of-care testing
- HIV home test.
Statistics from Altmetric.com
Introduction
Roughly 20% of HIV-infected individuals are unaware of their HIV status in France,1 while this proportion remains higher in other regions.2 These individuals constitute a major risk group contributing to the ongoing HIV epidemic, many of whom transmit their virus during acute HIV infection (AHI) (ie, 3 months after HIV acquisition).3 4
Rapid testing is known to increase HIV infection awareness for high-risk populations in point-of-care settings well after HIV transmission.2 Unfortunately, these tests often fail to diagnose HIV in patients with AHI. Previous assessments of rapid tests have been conducted during AHI,5 6 yet are limited to a handful of tests and none has assessed the performance of the STAT-VIEW HIV self-test.
In this retrospective study, we aimed to evaluate the sensitivity of the HIV self-test STAT-VIEW HIV1/2 Assay (Chembio Diagnostic Systems, Rungis, France), the only test authorised for at-home use in France (commercial name: AUTOTEST; AAZ Labs, Rungis, France), using samples collected from patients during the course of AHI. We compared test sensitivity to another rapid test (INSTI, bioLytical, Richmond, BC, Canada), commonly used in the Paris metropolitan public healthcare system. We then intended to report the clinical characteristics associated with a specimen producing a reactive test result during AHI.
Methods
Individuals presenting with AHI, defined by detectable HIV viral load (VL) and either non-reactive or indeterminate western blot (WB), at Saint-Antoine Hospital (Paris, France) were consecutively included in 2010–2015. Patients undergoing pre-exposure/post-exposure prophylaxis were excluded. Written informed consent was obtained from patients to use stored samples and personal data for non-interventional research.
Patient characteristics were obtained from computerised medical records. The estimated date of infection was based on patient-reported at-risk contact. If this date was unavailable, date of infection was defined as 10 days prior to symptom onset.7 Infection duration was estimated from the date of infection until the time of HIV diagnosis.
HIV antigen/antibody (ARCHITECT HIV 1/2 Ag/Ac Combo, Abbott Diagnostics, Rungis, France), p24 antigen (INNOTEST HIV Antigen mAb, Fujirebio Europe, Gent, Belgium), WB (NEW-LAV BLOT I, Bio-Rad, Marnes-la-Coquette, France) and plasma HIV-RNA VL (COBAS TaqMan HIV-1 Test, V.2.0, Roche Diagnostics, Rosny-sous-Bois, France; detection limit of 20 copies/mL) were performed at the Virology Department. Fiebig stages8 of AHI (table 1) were determined using virological and serological markers.
Comparing characteristics between patients with a reactive versus non-reactive STAT-VIEW rapid test during acute HIV infection
The STAT-VIEW HIV-1/2 assay, a third-generation immunochromatography-based self-test, detects antibodies recognising gp41 and gp120 antigens (HIV-1) and gp36 antigen (HIV-2). The INSTI, a third-generation flow-through HIV immunoassay, detects antibodies against recombinant proteins gp41 (HIV-1) and gp36 (HIV-2). Both tests were performed retrospectively according to manufacturer’s instructions on stored serum samples: 2.5 µL with STAT-VIEW and 50 µL with INSTI. Results were interpreted by two independent virologists.
Characteristics between patients with a reactive and non-reactive self-test were compared using Kruskal-Wallis test for continuous variables and Pearson χ² test or Fisher’s exact test for categorical variables. In an exploratory analysis, we modelled the probability of having a reactive test after HIV infection as a logistic function. The test result (reactive or non-reactive) was used as a dependent variable in a logistic regression model, while continuous time since estimated date of infection was included as the sole independent variable. Expected probabilities during infection and their 95% CIs were obtained from model parameters.
All data were deidentified, and only the principal investigator had access to identifying information. As the study was based on a convenience sample, no sample size calculation was performed. Statistical analysis was performed using STATA statistical software (V.12.1), and a p value of <0.05 was considered significant.
Results
A total of 50 patients met inclusion criteria, 10 of whom were not included because of concomitant pre-exposure/postexposure prophylaxis (n=2) or unavailable serum samples (n=8). Demographic, clinical characteristics and diagnostic results from routine laboratory examinations of the 40 included patients are given in table 1. Patients were predominately men (97.5%) who have sex with men (90%), presenting with acute HIV-associated illness (87.5%). Median estimated duration from infection to HIV diagnosis was 25 days.
Twenty-three patients (57.5%, 95% CI 40.9% to 73.0%) had a reactive STAT-VIEW test. Patients with a non-reactive versus reactive STAT-VIEW test (table 1) had a significantly shorter median time since infection (p=0.01), time since onset of symptoms (p=0.009), negative WB results (p<0.001), higher HIV-RNA VL (p=0.001), higher proportion with Fiebig stage III than IV (p=0.003) and lower CD4+ and CD8+ cell count (p=0.03 and p<0.001, respectively).
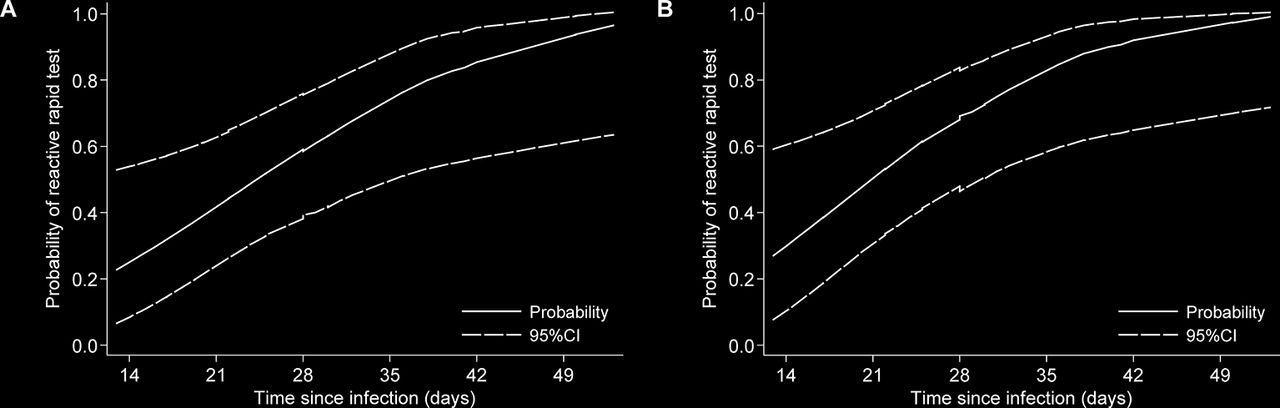
In order to understand test reactivity during the acute phase, we performed a post hoc analysis among patients with available data (n=37). The predicted probability of a reactive STAT-VIEW test became >50% after 24.3 days from suspected HIV transmission (figure 1A).
{kind=link}
Probability of reactive rapid tests during acute HIV infection. The probability of reactive STAT-VIEW (A) and INSTI (B) rapid tests were modelled separately using logistic regression. This probability is represented over the course of estimated HIV infection duration (solid line) along with 95% CIs.
Similarly, 25 patients (62.5%, 95% CI 45.8% to 77.3%) had a reactive INSTI test. Patients with a non-reactive versus reactive INSTI test (table 1) had a significantly shorter median time since infection (p=0.007), negative WB results (p=0.007), higher HIV-RNA VL (p=0.01), higher proportion with Fiebig stage III than IV (p=0.02), and lower CD4+ and CD8+ cell count (p=0.02 and p=0.002, respectively). The predicted probability of a reactive INSTI test became >50% after 20.9 days from suspected HIV transmission (figure 1B).
Discordant results were observed in six (15.0%) patients: four with a negative STAT-VIEW/positive INSTI and two with a positive STAT-VIEW/negative INSTI. For both tests, no between-reader discrepancies and no uninterpretable tests were observed.
Discussion
To the best of our knowledge, this study is the first to assess the performance of the STAT-VIEW rapid self-test using specimens from patients at the earliest stages of HIV infection. We observed that more than half of patients had a positive rapid test result despite having acute infection. This proportion was comparable when using the INSTI rapid test and falls in line with prior evaluations of other rapid tests among individuals with early HIV infection where sensitivities ranged from 54% to 93%.5 6
Some limitations need to be addressed. First, we only tested on serum samples, which may lend to more enriched concentrations of antibodies compared with capillary whole blood (as performed during self-testing). Test sensitivity reported in our study could have been inflated; however, this bias is more pertinent to small volume, lateral flow tests than for flow-through tests.9 Second, tests were performed by trained virologists. Similar test performance has been observed among self-test users, suggesting that this bias would have little effect on our study.10 Nevertheless, tests were performed under ideal storage conditions (ie, directly after purchase and prior to its expiration date), which might not be the case for at-home use. Finally, duration of HIV infection was not determined by serial sampling, while establishing the date of transmission from consecutive negative to positive serology. Despite every attempt made to ensure the most accurate date of HIV acquisition was used, we cannot exclude improper estimation of HIV infection duration.
Despite these limitations, we were able to characterise the relationship between test sensitivity and the timing of testing after HIV acquisition. From the logistic regression model applied in our study, test sensitivity steadily increased over reconstructed HIV infection with 76% and 85% of infections detected at 5 weeks from transmission using the STAT-VIEW and INSTI tests, respectively. In addition, non-reactive results were significantly associated with higher HIV-RNA VL and lower CD4+ and CD8+ cell count. These parameters naturally correspond to earlier stages of infection, as reflected by the higher proportion of non-reactive tests in patients with Fiebig stage III and negative WB results. It should be mentioned that the rapid tests used in our study were third generation, which rely on antibody detection alone. Fourth-generation tests, detecting both antibody and antigen, could have higher sensitivities and consequently shorten the window of detection reported in our study.
Flow-through rapid tests, much like any enzyme immunoassay, are able to detect anti-HIV antibodies within 25–35 days after infection, closely following what would be expected from the model above.11 Although rapid testing is not recommended during the acute phase, the fairly high sensitivity observed in our study would suggest that there could be some benefit with its use during AHI, particularly after 5 weeks from infection. Individuals conducting home testing with the STAT-VIEW could be cautioned to not rely on a negative result to accurately exclude HIV infection within at least 5 weeks of their last potential exposure to HIV. Nevertheless, the full implications of a non-reactive test would be uncertain and need further consideration.
In conclusion, the STAT-VIEW rapid test intended for at-home use was able to detect at least 75% of HIV infections when performed on serum collected at least 5 weeks after HIV transmission. Although nucleic acid testing will remain the mainstay of HIV diagnosis, especially during AHI, these results suggest that rapid tests could serve some utility in detecting HIV even during the early stages of infection. The extent of this benefit still needs to be determined in general (especially when using blood specimens from fingerstick sampling), within specific at-risk groups, and for individuals with delayed HIV seroconversion due to pre-exposure or postexposure prophylaxis.
Acknowledgments
AAZ Labs (Rungis, France), which acts as a rapid test distributor, kindly provided all STAT-VIEW HIV1/2 Assay home-tests for a market value of €480. A postdoctoral fellowship was awarded by Sidaction to AB, providing paid salary under a temporary contract with the Institut national de la santé et de la recherche médicale (Inserm). We would like to greatly thank all patients for their participation and the employees of the Virology Department and Department of Infectious and Tropical Diseases at Saint-Antoine Hospital for their assistance.
Footnotes
Handling editor Jackie A Cassell
Contributors We confirm that all authors have seen and approved the content and have contributed significantly to this work. NW was responsible for locating stored samples, performing rapid tests and gathering biological data. NB was responsible for overseeing interpretation of data and drafting and revising the article. JB was responsible for gathering clinical data and gave critical revisions to the manuscript. AB performed statistical analysis and drafted parts of the manuscript. LM-J designed and oversaw the study and critically revised the article. P-MG oversaw the study and gave critical revisions of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors confirm that, for approved reasons, some access restrictions apply to the data underlying the findings. The data cannot be publicly available due to legal and ethical restrictions from the French Authority (Commission nationale de l’informatique et des libertés). Requests for data use can be made to the corresponding author of the study (Narjis Boukli at narjis.boukli@aphp.fr).