Article Text

Abstract
Objectives New molecular techniques have allowed describing groups of bacterial communities in the vagina (community state types (CST)) that could play an important role in Chlamydia trachomatis (CT) infection. Our aim was to describe the distribution of CST in a population of young women in France.
Methods A cross-sectional study was carried out in June 2015 among anonymous young women attending a STI clinic in Bordeaux, France. Participants provided a vaginal sample for CT screening and sociodemographic data. CT was diagnosed using the Aptima-combo 2 transcription-mediated-amplification assay. Vaginal microbiota composition was characterised using 16S rRNA gene amplicon sequencing.
Results Microbiota composition and CT status were available for 132 women. CST dominated by Lactobacillus crispatus (CST-I), L. iners (CST-III) and a diversity of anaerobes (CST-IV) represented 37.1%, 38.6% and 22.0% of the sample, respectively. Twenty-one out of 132 women were CT positive. Proportions of CT-positive women were higher for samples belonging to CST-III (21.6%) and CST-IV (17.2%) than to CST-I (8.2%).
Conclusions Five CST were found in 132 young women from a STI clinic in France. These CSTs were not significantly associated with CT but higher proportions of CT-positive women were found in CST-III and CST-IV, consistent with a previous study in the Netherlands. Though our study lacked statistical power and was cross-sectional, it is a necessary first step to understand the structure of the vaginal microbiota in French women with or without infection before performing in-depth longitudinal studies.
- community state type
- lactobacillus
- 16S rRNA gene
- microbiota
- microbial consortia
- chlamydia trachomatis
- (bacterial) sexually transmitted infections
- vagina
- bacterial vaginosis
Statistics from Altmetric.com
- community state type
- lactobacillus
- 16S rRNA gene
- microbiota
- microbial consortia
- chlamydia trachomatis
- (bacterial) sexually transmitted infections
- vagina
- bacterial vaginosis
Introduction
The vaginal microbiota, in particular Lactobacillus spp., is thought to play a major role in preventing STIs through mechanisms such as ecological competition, the production of lactic acid and antimicrobials such as bacteriocins.1 2 Using culture-independent methods, groups of bacterial communities have been described in the vagina (community state types (CST)).3 Four CSTs are often dominated by Lactobacillus spp. (CST-I: L. crispatus; CST-II: L. gasseri; CST-III: L. iners; CST-V: L. jensenii) and one CST has low or no Lactobacillus spp. and a wide array of strict and facultative anaerobes (CST-IV). These CSTs are hypothesised to differentially affect the risk to STIs.
Genital infection with Chlamydia trachomatis (CT) is the most reported bacterial STI worldwide,4 in particular among young women. Though mostly asymptomatic, this infection can progress towards pelvic inflammatory disease (PID), which, if left untreated, is associated with tubal factor infertility and ectopic pregnancy.5 The last estimate of CT positivity in France was 8.3% among women aged 18–24 years in 2012.6 Throughout the course of CT, many factors are likely to play a role in modulating the risk of infection, persistence and progression towards PID, including the composition and function of the vaginal microbiota.
Here, we sought to characterise the vaginal microbiota in consecutive women attending a STI clinic in Bordeaux, France, and compare our results with previous findings.
Methods
Design and study population
A cross-sectional study was carried out in June 2015 that aimed at characterising the vaginal microbiota composition in young women attending a STI clinic in Bordeaux, France. Participants provided a single self-collected vaginal sample for routine CT screening and sociodemographic data such as age, place of birth and reasons for consultation.
CT screening and vaginal microbiota characterisation
Vaginal samples were kept in Aptima (Hologic) medium allowing transportation at room temperature. CT screening was carried out at the CT National Reference Centre using the Aptima-combo 2 transcription-mediated-amplification assay. A 200 µl aliquot of the samples was centrifuged and resuspended in 300 µl of MoBio Microbiome Kit (MoBio/Qiagen) lysis buffer and processed according to the manufacturer’s recommendation. The DNA was eluted in 100 µl of elution buffer. Vaginal microbiota composition was characterised using 16S rRNA gene amplicon sequencing on an Ilumina MiSeq platform (San Diego, California, USA) using the 300 paired-end protocol. A total of 50 ng of DNA was subject to PCR amplification of the V3–V4 region of the 16S rRNA gene using a dual-indexing approach previously published.7 Sequence reads were processed and taxonomic assignments were performed on each assembled sequence using PECAN, a novel and rapid taxonomic classifier that affords classification of all sequence reads (ravel-lab.org/pecan).
CST clustering and statistical analysis
Women were grouped into CSTs using hierarchical clustering. The clustering was implemented in R statistical package ‘stats’ using Ward linkage hierarchical clustering based on Jensen-Shannon divergence metrics. CT-positive women and CT-negative women were compared using Fisher-exact test. Statistical analyses were performed using Stata V.12.0 and R V.3.3.0.
Attendance at the STI clinic is completely anonymous. The samples and data used in this research were collected as part of routine care. Oral consent was obtained from participants, after providing information on this use. The electronic database is hosted with the authorisation of the French National Commission for Computed Data and Individual Freedom.
Results
Sociodemographic characteristics
A total of 151 women were recruited in the STI clinic in Bordeaux and provided vaginal samples for CT diagnosis and vaginal microbiota characterisation, of which 132 yielded workable results.
Age was available for 119 women and ranged from 16 to 33 years. Out of 116 women for which the origin was available, 87.9% were born in Metropolitan France, whereas the rest of them were born abroad or in overseas French departments. Main reasons for the visit were ‘at risk intercourse’ (20.5%), ‘problem in condom use’ (19.7%), ‘before stopping condom use’ (19.7%), ‘change of partner’ (13.7%) and ‘symptoms’ (6%).
Vaginal microbiota composition
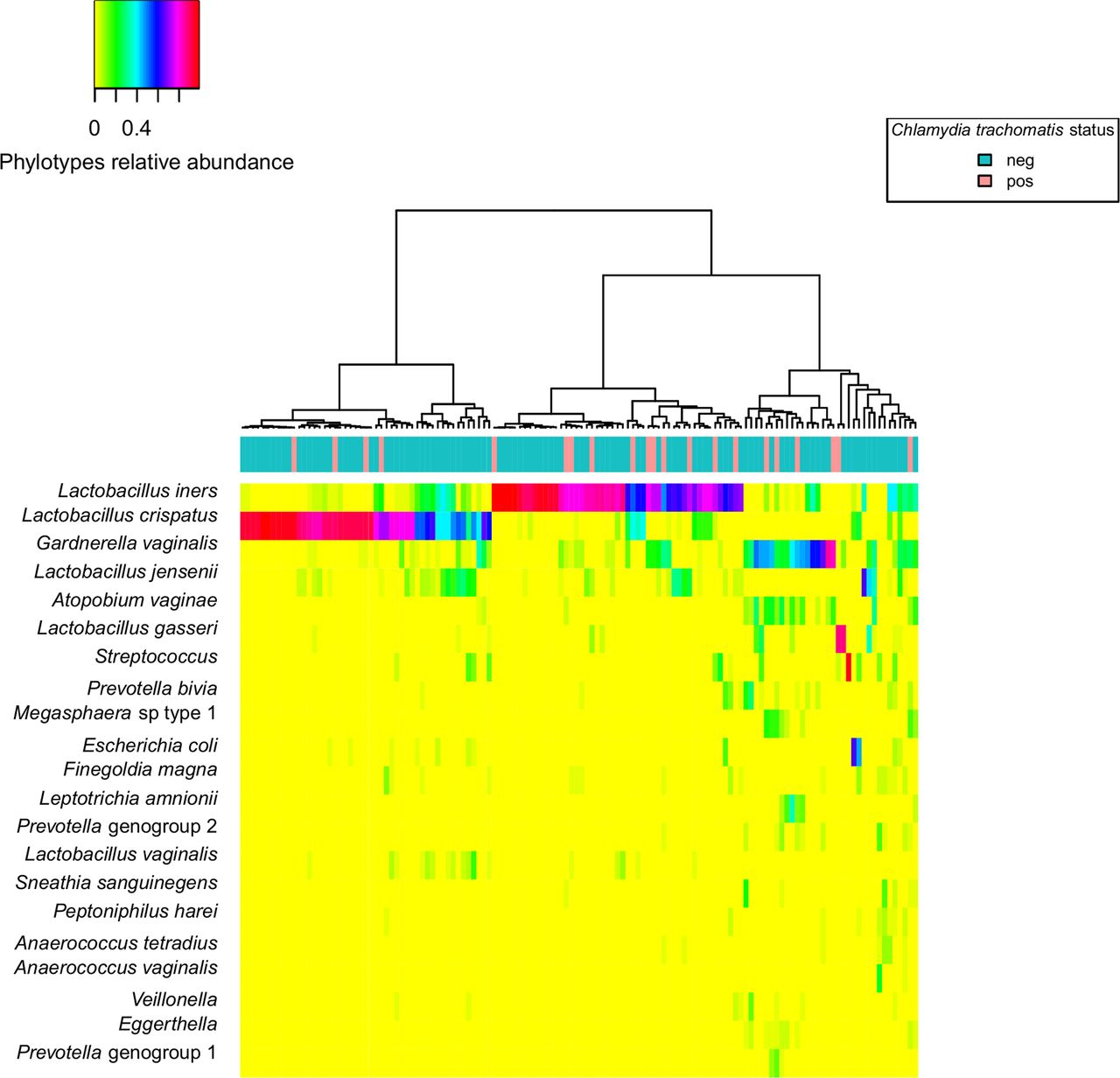
CSTs dominated by L. crispatus (CST-I), L. iners (CST-III) or lacking Lactobacillus spp. and comprising a wide array of strict and facultative anaerobes (CST-IV) represented 37.1%, 38.6% and 22.0% of the samples, respectively (figure 1 and online Supplementary table 1). Only a few samples were assigned to CST-II and CST-V. L. crispatus was either present in very low or high proportion of the vaginal microbiota, accounting for up to 97% of the microbiota for some women. Similarly, the proportion of L. iners in some women reached 98%. Among CST-IV communities, no single bacteria dominated the vaginal microbiota, but both Gardnerella vaginalis and Atopobium vaginae were commonly found.

{kind=link}
Heatmap of relative abundance of microbial taxa found in the vaginal bacterial communities of 132 young women from a STI clinic in France, June 2015.
Within CST-I and CST-III, two subgroups could be highlighted, one for which the Lactobacillus spp. was highly dominant (CST-IA and CST-IIIA) and one for which it was dominant but other taxa were present at low abundance (CST-IB and CST-IIIB) (figure 1).
CT infection
Twenty-one women (15.9%) out of 132 were CT positive. All CT-positive women were aged 18–24 years. Proportions of CT-positive women were higher in CST-III (21.6%, 11 out of 51) and CST-IV (17.2%, five out of 29) than in CST-I (8.2%, four out of 49). CST-I represented 19.1% in CT-positive women and 40.5% in CT-negative women, while these proportions corresponded to 52.4% and 36.0 for CST-III and 23.8% and 21.6% for CST-IV (online Supplementary table 1).
ORs of being CT positive were 3.09 (95% CI 0.91 to 10.49) for CST-III compared with CST-I and 2.34 (95% CI 0.58 to 9.55) for CST-IV compared with CST-I, though these results were not statistically significant.
Discussion
The high proportion of CT-positive women in our study (15.9%) is probably due to the fact that study participants represented a group of relatively high-risk women, compared with the general population. CT positivity was much higher than the last estimate in France, in a web-based study in 2012 where 8.3% of women aged 18–24 years in the general population were found positive for CT.6 All women infected with CT were aged 18–24 years, which corresponds to the age group most affected by this infection.
The vaginal microbiota of young women was characterised using culture-independent methods for the first time in French women. Five CSTs could be described in these 132 young women attending a STI clinic in France, with the three main CSTs being divided into two subgroups each according to community diversity. CSTs were not significantly associated with C. trachomatis status but higher proportions of CT-positive women were found in CST-III and CST-IV than in CST-I.
In a previous study by Ravel et al,3 the five CSTs were found at a frequency of 26.2%, 6.3%, 34.1%, 27.4% and 5.3% for CST-I, CST-II, CST-III, CST-IV and CST-V, respectively, in healthy CT-negative women from Baltimore and Atlanta in the USA. Similar to our findings in CT-negative women, CST-I, CST-III and CST-IV were the most prevalent vaginal microbiota types found in this population, though our study showed a higher proportion of CST-I in non-infected women. This over-representation of CST-I in non-infected women could be explained with an increased protection to STIs by a community dominated by L. crispatus as previously hypothesised by van der Veer et al.8 In their study of a high-risk population for STIs in the Netherlands, proportions of CST-I, CST-III and CST-IV in CT-negative women were 39.0%, 26.8% and 34.2%, respectively. Among CT-positive women, the distribution of CSTs in our study was somewhat similar to that found by van der Veer et al (online Supplementary table 1), except for CST-IV. This CST represented 48.1% of CT-positive women, while in our study it accounted for only 23.8%. Our results in French women are similar to the study of van der Veer et al hypothesising a detrimental role of CST-III and CST-IV. Altogether, these data point to a protective role of CST-I, dominated by L. crispatus, and a potential increased risk for CT infection for women with CST-III and CST-IV, which might vary by population. One can speculate that these microbiota types are associated with increased susceptibility; however, it cannot be excluded that the infection itself results in CST-III and CST-IV vaginal microbiota. Epidemiological studies, using the Nugent score, a Gram stain and microscopy-based evaluation of the microbiota, have shown that high Nugent score is a risk factor for CT, Neisseria gonorrhoeae and HIV infection.2 9
The cross-sectional study design of the current study and the relatively small sample size are a limitation. Further studies with prospective longitudinal study design would afford determining whether the vaginal microbiota predisposes to CT infection, or whether CT infection modifies the composition of the vaginal microbiota and would allow to account for the dynamics structure of the vaginal microbiota over time previously reported.10 Finally, analysis of the vaginal microbiota would strongly benefit from information on sexual practices, personal hygiene, gynaecological history or concurrent treatment, in particular oral contraceptive and antibiotic use, information we did not have access to in this study. Nonetheless, this study is a first necessary step to inform the design of larger prospective longitudinal studies.
Acknowledgments
We would like to thank all the participants of this study, the Centre Gratuit d’Information, de Dépistage et de Diagnostic (CeGIDD) of Bordeaux, France, and all the staff who were involved in this study. The National Reference Center for bacterial sexually transmitted infections is gratefully acknowledged.
Footnotes
Handling editor Jackie A Cassell
Contributors JT was a major contributor in data analysis, with support from AT, JR and ED-A. JT wrote the manuscript. BdB, ILH, CB and ED-A were major contributors in the conception of the study. BdB and JR were major contributors in biological and bioinformatics analyses. All authors read and approved the final manuscript.
Funding This study was funded by the 2013 Institut National du Cancer, Institut de Recherche en Santé Publique (INCa-IReSP) call for projects ‘Recherche Prévention Primaire’ (Reference number: A15012LS).
Competing interests None declared.
Ethics approval CNIL registration number: 1928790.
Provenance and peer review Not commissioned; externally peer reviewed.