Article Text

Abstract
Background Men who have sex with men (MSM) are disproportionately affected by HIV and other STIs worldwide. Rectal douching, which is commonly used by MSM in preparation for anal sex, may increase the risk of HIV and other STIs by injuring the rectal mucosa. Results from individual studies reporting associations between rectal douching and HIV and other STIs among MSM are inconsistent. We performed a systematic review and meta-analysis to estimate the association between rectal douching and HIV and other STIs among MSM.
Methods We searched PubMed, Embase, Scopus and Web of Science for studies published from January 1970 to November 2018. Studies that reported ORs and 95% CIs of associations between rectal douching and infection with HIV/STIs, or reported enough data to calculate these estimates, were included. We assessed risk of bias using the Newcastle-Ottawa Scale. ORs were pooled using a random effects model.
Results Twenty-eight eligible studies were identified in our review, of which 24 (20 398 participants) were included in the meta-analysis. Rectal douching was associated with increased odds of infection with HIV (OR 2.80, 95% CI 2.32 to 3.39), and any STI other than HIV (including hepatitis B virus (HBV), hepatitis C virus (HCV), chlamydia, gonorrhoea, syphilis and human papillomavirus) (OR 2.46, 95% CI 1.95 to 3.11) among MSM. For specific STIs, douching was associated with increased odds of viral hepatitis (HBV, HCV) (OR 3.29, 95% CI 2.79 to 3.87), and chlamydia or gonorrhoea (OR 3.25, 95% CI 2.02 to 5.23). These associations remained significant in studies that adjusted for potential confounders.
Conclusion Rectal douching may put MSM at increased risk for infection with HIV and other STIs. Longitudinal studies are needed to clarify this association, and health education materials should inform men of the potential for increased risk of infection with rectal douching.
- rectal douching
- enema
- men who have sex with men
- HIV
- sexually transmitted infections
- meta-analysis
Statistics from Altmetric.com
Key messages
Currently, there are no definitive estimates of association between rectal douching and HIV and other STIs among men who have sex with men.
This systematic review found men who ever douched have greater odds to be infected with HIV and other STIs.
Health education materials that inform men of the potential for increased risk of infection with rectal douching are urgently needed.
Introduction
Men who have sex with men (MSM) are disproportionately affected by HIV and other STIs worldwide.1–3 Although HIV pre-exposure prophylaxis (PrEP) is efficacious in preventing HIV transmission among HIV-negative MSM,4 PrEP remains unavailable in many countries of low and middle income where the burden of HIV/STI epidemic in MSM is particularly heavy.5–7 MSM who engage in receptive anal sex are particularly vulnerable.8 The rectum’s single-cell epithelium is susceptible to tears and abrasions during anal sex, facilitating transmission of HIV and other STIs.9 Therefore, more evidence-based strategies to prevent HIV and other STIs among MSM are urgently needed.
Rectal douching involves inserting a liquid (eg, tap water, soapsuds) into the anus by means of some tool to facilitate defecation and cleanse the rectum. This behaviour is common among MSM before and after anal sex. The proportion of MSM practising rectal douching ranges from 29.8% to 52.0% in the USA,10–12 18.2%–27.0% in Peru13 14 and 13.5%–46.3% in the Netherlands.15 16 Among men reporting a history of douching, 63.5%–90.9% and 27.4%–46.6% performed rectal douching before and after anal sex, respectively.11 13 17 Reasons for douching identified by MSM include increased hygiene,11 13 17 18 enhanced sexual pleasure11 13 17 18 and STI prevention.11 Factors such as preferred sexual position, age and income have been found to be independently associated with douching behaviour.11 13 15
It is biologically plausible that rectal douching may increase risk of infection with HIV and other STIs. The rectum’s single-celled epithelium may be damaged by friction and stimulation that result from douching, thereby allowing for pathogen entry.9 Nevertheless, reported associations between HIV/STIs and rectal douching among MSM are inconsistent. Several studies conducted in the USA found that MSM who practise rectal douching were more likely to be infected with HIV,10 11 hepatitis B virus (HBV),10 chlamydia12 and gonorrhoea.12 In the Netherlands, two studies reported that douching may increase risk for chlamydia and gonorrhoea infection,16 19 while a third study found no difference in prevalence of chlamydia and gonorrhoea comparing MSM who do and do not practice rectal douching.15 Reports from South America and Thailand have shown that douching was not associated with increased risk of HIV and human papillomavirus (HPV) infection.13 17 20 It remains unknown that whether the risk of HIV/STI infection is affected by douching timing (before or after anal sex), duration, and types and volume of liquids used for douching.
The uncertain relationship between rectal douching and risk of HIV/STIs has contributed to confusion and the circulation of misinformation that rectal douching prevents HIV/STI infection during anal sex in MSM communities.11 21 To inform global HIV/STI prevention strategies for MSM, we conducted a comprehensive systematic review and meta-analysis to estimate the associations between rectal douching and HIV and other STIs among MSM.
Methods
Literature search
Two authors (PL and HZ) independently conducted this systematic review and meta-analysis in accordance with PRISMA guidelines.22 23 We searched PubMed, Embase, Scopus and Web of Science for studies published from January 1970 to November 2018. Search terms were enema and MSM with their synonyms ([“enema,” “douching,” “douche,” “clysma,” “clyster,” “enteroclysis,” OR “rectal cleanliness.”] AND [“men who have sex with men,” “MSM,” “homosexual,” OR “gay.”]). References of identified articles were screened for additional titles meeting criteria for inclusion. Studies of all designs that contained quantitative data on the prevalence of rectal douching, HIV and other STIs (eg, HBV, syphilis, chlamydia, gonorrhoea) among MSM were considered for full-text review. If multiple publications reported results from a single original study, data were only extracted from the single most comprehensive publication.
Quality assessment
We assessed risk of bias of included studies using the Newcastle-Ottawa Scale (NOS) for cohort and case–control studies and an adapted NOS for cross-sectional studies.24 25 Risk of bias was assessed across three categories: selection of subjects (four items), comparability between groups (two items) and assessment of outcome or exposure (three items). Studies meeting more than half of all items were considered lower risk of bias (online supplementary table S1).
Supplemental material
Data extraction and meta-analysis
We extracted the following information from eligible publications: study characteristics (first author, publication year, study period, study location and recruitment setting), characteristics of douching behaviour (reasons for douching, types of douching liquids used, douching tools and douching duration), method used to determine HIV/STI status (self-reported or laboratory confirmed infection), proportion of MSM with high-risk sexual behaviours among those who douched, and douching prevalence. ORs and their 95% CIs for the association between douching and infection with HIV and other STIs in MSM were also extracted, with priority given to ORs that adjusted for potential confounders. For studies that did not report ORs, raw four-table data were extracted to compute crude ORs and their 95% CIs.
Pooled ORs and their 95% CIs were estimated using a random effects model.26 For STIs other than HIV, we first calculated the association between rectal douching and any STI other than HIV as a single composite outcome using the formula developed by Borenstein et al .27 We then calculated pooled ORs for associations between douching and specific STIs (viral hepatitis, chlamydia or gonorrhoea). To detect potential outliers, we conducted sensitivity analyses in which studies were iteratively omitted and pooled estimates were recalculated.
Test of heterogeneity and publication bias
Statistical heterogeneity was assessed using both Cochran’s Q tests (p<0.10 was defined as significant heterogeneity) and I2 index (I2 <25%, 25%–75%, >75% were defined as low, moderate and high heterogeneity, respectively).28 29 We explored potential sources of heterogeneity across included studies with univariate meta-regression and subgroup analyses in which studies were stratified based on study characteristics, method used to determine HIV/STI status and type of association estimate reported (adjusted OR or unadjusted OR). We visualised publication bias using Egger’s regression test and funnel plots.30 31 All statistical analyses were performed using Stata V.14.0 (Stata Corporation, College Station, Texas, USA).
Results
Study characteristics
A total of 361 relevant abstracts were identified through our search, and 49 studies were selected for full-text review (figure 1). Twenty-eight articles were eligible for inclusion.10–13 15–17 19–21 32–49 Characteristics of included studies are summarised in table 1. The risk of bias of included studies, based on the NOS, was low to moderate (median quality score=63%, IQR 50%–75%), with 20 (71.4%) studies that met more than half of all items being considered lower risk of bias (table 1, online supplementary table S1). Among all included studies, 13 (46.4%) were conducted in North America, 2 (7.1%) in South America, 10 (35.7%) in Europe, 2 (7.1%) in Asia and 1 (3.6%) in Africa. Most were cross-sectional (71.4%), and over half recruited study subjects through hospitals or clinics (60.7%).
Study characteristics of included publications

Flow diagram of article selection strategy. MSM, men who have sex with men.
A total of 21 570 MSM were included in our review, 43.7% of whom reported a history of rectal douching. The proportion of men practising rectal douching in individual studies ranged from 13.5% to 70.5% (median, 52.0%). Among men reporting a history of douching, the proportion of men who engaged in unprotected anal intercourse (UAI) ranged from 7.9% to 61.7% (median, 52.1%), and men having six or more sex partners during the last 6 months ranged from 58.0% to 74.4% (median, 58.0%).
Of the 28 included studies, 20 assessed the association between rectal douching and HIV infection,10–13 15 17 20 21 33 34 36 37 39 41–44 46 48 49 and 17 examined associations between douching and any STI other than HIV (HBV, hepatitis C virus (HCV), chlamydia, gonorrhoea, syphilis and HPV).10–12 15–17 19 20 32 35–40 45 47 Among the 20 studies reporting HIV infection, 17 found a positive association between douching and HIV infection,10–12 15 21 33 34 36 37 39 41–44 46 48 49 while three found no association with HIV infection.13 17 20 Among the 17 studies that reported the prevalence of an STI other than HIV, three studies found rectal douching to be associated with greater odds of infection with HBV,10 36 45 one for HCV,32 six for chlamydia and gonorrhoea,12 16 19 38 40 47 and one for syphilis.36 Two reported a significant association between douching and infection with most STIs (including chlamydia, gonorrhoea, syphilis, HCV and HPV).11 37 Four reported no statistically significant association between douching and HBV,35 39 chlamydia, gonorrhoea15 and HPV infection,20 and one reported no association for most STIs.17 Four studies (three for HIV and one for other STIs) were excluded from the meta-analysis due to insufficient data to compute ORs and their 95% CIs.35 42 44 46
Meta-analysis of associations between rectal douching and HIV/STIs
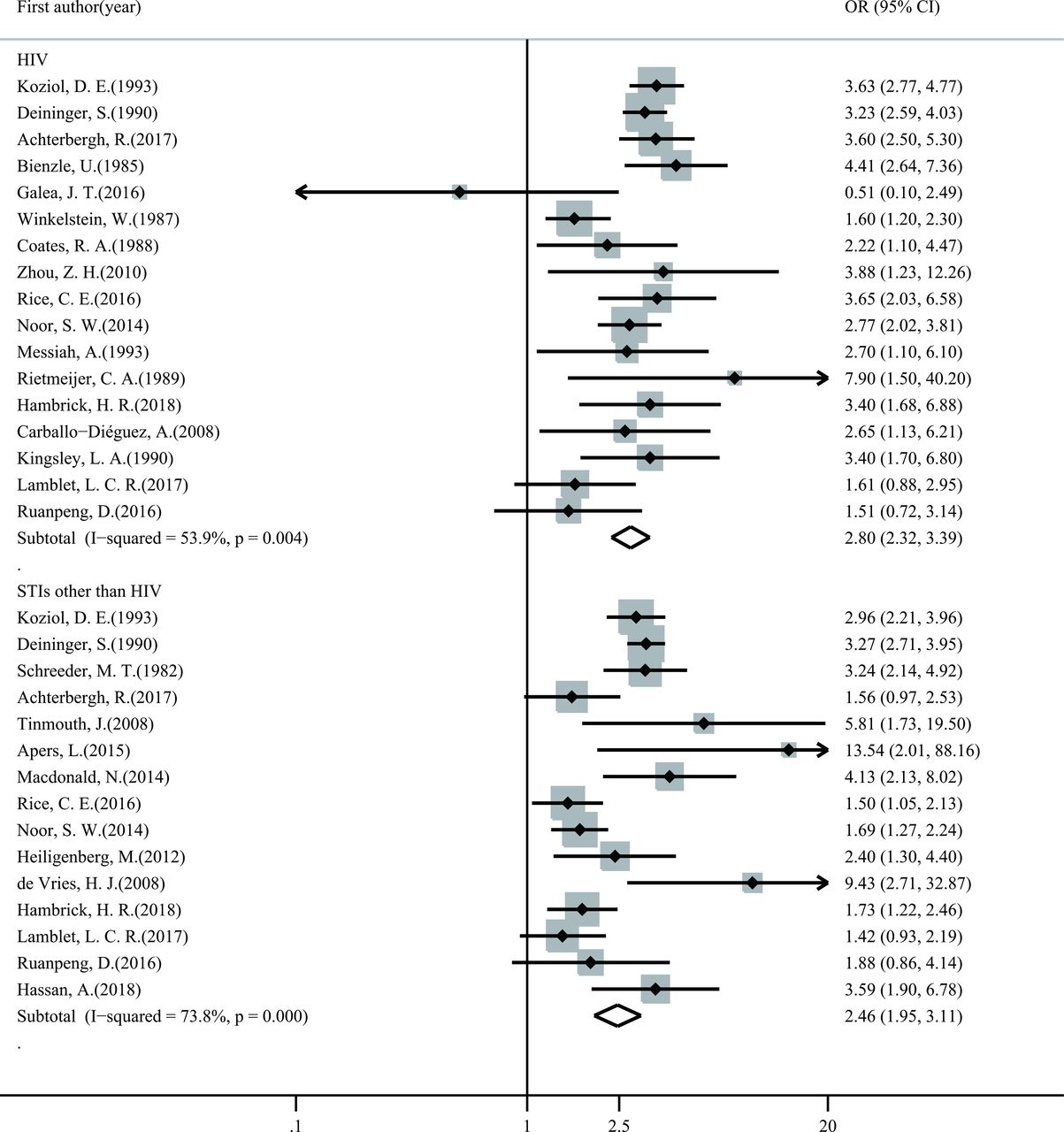
In meta-analysis, MSM who reported rectal douching were more likely to be living with HIV (OR 2.80, 95% CI 2.32 to 3.39; figure 2). Estimates had moderate heterogeneity (I2=53.9%, Q test p<0.01). In univariate meta-regression analysis, study design (cross-sectional studies vs cohort studies, R2=91%; table 2) explained the variation between studies (p<0.05). The odds of infection with HIV among MSM who practised douching was higher in cross-sectional studies compared with cohort studies (OR 1.76, 95% CI 1.15 to 2.71).
{kind=link}
{kind=link}
Forest plot of ORs for HIV and other STI infections comparing MSM who do and do not practise rectal douching.
Subgroup analysis and univariate meta-regression for odds of HIV/STIs infection comparing MSM who do and do not practise rectal douching
In subgroup analysis, the association between douching and HIV infection remained significant in studies that adjusted for potential confounders (OR 2.74, 95% CI 2.14 to 3.50, I2=46.0%). Douching was not associated with increased risk of HIV infection in cohort studies (OR 1.77, 95% CI 0.85 to 3.70, I2=67.1%), studies conducted in South America (OR 1.17, 95% CI 0.42 to 3.21, I2=41.9%) and studies conducted in Asia (OR 2.17, 95% CI 0.88 to 5.35, I2=45.5%) (table 2).
Among the 15 studies that reported associations between rectal douching and other STIs, pooled ORs showed MSM who practised rectal douching had higher odds of infection with any STI other than HIV (OR 2.46, 95% CI 1.95 to 3.11; figure 2). Odds of infection with viral hepatitis (HBV, HCV) (OR 3.29, 95% CI 2.79 to 3.87) and chlamydia or gonorrhoea (OR 3.25, 95% CI 2.02 to 5.23) were higher among MSM who reported douching (table 2). Heterogeneity was moderate across studies reporting any STI other than HIV (I2=73.8%) and chlamydia or gonorrhoea (I2=61.2%) as outcomes, but was not detected in studies that reported viral hepatitis infection (I2=0.0%). In univariate meta-regression analysis, study period (after 2011 vs 2001–2010, R2=100%) and method used to determine STI status (laboratory confirmed vs self-reported infection, R2=45%) explained the variation between studies (p<0.05). The risk of infection with any STI other than HIV among MSM who practised rectal douching was higher in studies conducted after 2011 (OR 0.44, 95% CI 0.27 to 0.72) compared with studies conducted between 2001 and 2010.
In subgroup analysis, the direction of pooled effect sizes was consistent across subgroups (table 2). The association between rectal douching and infection with any STI other than HIV was stronger in studies conducted before 1990 (OR 3.18, 95% CI 2.75 to 3.69, I2=0.0%) and during 2000–2010 (OR 4.03, 95% CI 2.35 to 6.88, I2=36.6%) compared with studies conducted after 2010 (OR 1.76, 95% CI 1.43 to 2.18, I2=38.0%). The magnitude of this association was also stronger in studies where infection was laboratory confirmed (OR 2.83, 95% CI 2.20 to 3.64, I2=65.3%) compared with self-reported (OR 1.64, 95% CI 1.35 to 2.00, I2=0.0%). The association between douching and any STI other than HIV remained significant in studies that adjusted for potential confounders (OR 2.27, 95% CI 1.70 to 3.04, I2=66.9%).
Sensitivity analysis and publication bias
In sensitivity analysis, none of the pooled association estimates were affected by removal of any one study (online supplementary figure S3, S4). We did not find evidence of publication bias in funnel plots and Egger’s tests performed for all comparison models (online supplementary figure S1, S2).
Discussion
In this systematic review and meta-analysis, we found MSM who practise rectal douching were more likely to be living with HIV compared with MSM who do not douche. This association remained significant in studies that adjusted for potential confounders. Men who douched also had higher odds of infection with any STI other than HIV, including viral hepatitis (HBV, HCV), chlamydia, gonorrhoea and syphilis. This association was stronger in studies where infection was laboratory confirmed compared with self-reported. Our results contribute to the existing literature by reporting the first pooled estimates of associations between rectal douching and HIV and other STIs among MSM.
Our findings were in line with the biological plausibility that rectal douching may increase susceptibility for HIV/STI transmission through sloughing rectal epithelium.9 Particularly, liquids used while douching, including tap water, soapsuds, and hyperosmolar enemas,11 17 50 can denude the rectal epithelium,51–53 and large volume enemas can produce rectal trauma.53 Improper use of douching tools may also increase risk of mucosal injury, and pathogens may be transmitted through shared douching equipment contaminated with blood or bodily secretions.32 Furthermore, douching may remove bacterial flora necessary to maintain a healthy rectal microbiome, leading to mucosal inflammation and facilitating pathogen entry.17 43
Despite previous research suggesting that rectal douching may increase this risk of HIV and STI transmission, this is the first systematic review and meta-analysis known to these authors to quantify associations between rectal douching and HIV/STIs among MSM. A previous review focused on behavioural aspects of douching among both men and women, but did not investigate associations with HIV or other STIs.54 In our meta-analysis, we focused exclusively on MSM, a population at higher risk of infection with HIV/STIs and with higher prevalence of rectal douching compared with women.
Among MSM included in our review, 8060 (43.7%) reported a history of rectal douching, 12 175 (71.5%) engaged in receptive anal sex and 2989 (40.3%) reported a history of UAI. These risk behaviours often occur together, with a high proportion of MSM who douche also reporting history of UAI,11 15 group sex37 and greater number of sex partners.11 13 This co-occurrence of risk factors likely contributes to persistently high rates of HIV/STI infection in this population,6 55 and may also confound associations between douching and risk of infection with HIV/STIs. However, most studies included in this meta-analysis performed multivariable logistic regression to adjust for potential confounders when estimating associations between douching and infection with HIV (12 of 17 studies) and other STIs (9 of 15 studies). In subgroup analysis, studies that adjusted for confounding found that men who douched continued to have greater odds of infection with HIV, viral hepatitis (HBV, HCV), and chlamydia or gonorrhoea. Additionally, more than half of studies (71.4%) included in this review were of low risk of bias, and the associations between rectal douching and increased odds of HIV/STIs persisted in studies with different periods of recall and studies where infection was laboratory confirmed. Therefore, the observed associations between douching and HIV/STIs are not simply the result of confounding risk behaviours. High rates of co-occurring risk behaviours, including rectal douching, also highlight the need to explore high-risk practices among MSM in a holistic way that accounts for the complex realities of the sexual risk environment.
Notably, awareness of potential risks of rectal douching was low among MSM, and some men even held the unsubstantiated view that rectal douching can reduce HIV/STI transmission by washing away pathogens.11 21 In light of our finding that rectal douching was associated with higher odds of HIV infection, future educational efforts should warn MSM about the potential for increased risk of infection if they practise douching. Additionally, previous studies have demonstrated that microbicide rectal enemas may become a promising vehicle for the delivery of HIV PrEP, which would both aid in preparation for anal sex and offer protection from HIV/STIs.56 57 More studies are needed to investigate the protective effect of microbicide enemas against HIV/STIs and assess MSM willingness to use microbicide enemas.
Findings from this review should be considered in light of several limitations. First, this meta-analysis was based on data extracted from observational studies, none of which were designed to resolve issues of temporality, preventing us from drawing conclusions regarding the causal relationship between rectal douching and HIV/STIs. Second, the majority of included studies (37.5%) were conducted in the USA, limiting generalisability of our results to MSM in other regions. Further research in low-income and middle-income countries is needed to clarify the relationship between rectal douching and HIV/STI transmission among MSM more generally. Third, few studies reported data on transgender women; consequently, we were unable to explore this group separately from MSM. Fourth, most studies (66.7%) did not differentiate between douching before and after anal sex, and only one (4.2%) study reported association estimate between douching after anal sex and HIV, limiting our ability to compare the risks of infection associated with these two distinct douching practices. Fifth, none of the studies identified by this review reported differences in the odds of HIV/STI infection comparing diverse types and volume of liquids for douching, precluding study of possible influencing factors. Lastly, only a few studies were included in several subgroup analyses for the association between douching and HIV, and few included studies reported data describing associations between rectal douching and STIs other than HIV, which limited statistical power for portions of our meta-analysis. Findings from these meta-analyses should be considered preliminary and should be further investigated when more data become available.
We found rectal douching to be associated with increased odds of infection with HIV and other STI among MSM. Because the data used to estimate pooled ORs in this meta-analysis were largely extracted from cross-sectional studies, more rigorously designed longitudinal studies are needed to determine whether there is a causal relationship between rectal douching and HIV/STIs among MSM. Future studies should account for the possible contributory factors, including timing of douching (before or after anal sex), types and volume of liquids used, douching duration and use of associated tools. More studies are also needed to examine co-occurring high-risk sexual behaviours among MSM who practise rectal douching. Our results suggest the need for health education materials that inform MSM about the potential for increased risk of HIV/STIs if they choose to douche before or after anal sex.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Acknowledgments
We thank Darin Ruanpeng, Research Institute for Health Sciences, Chiang Mai University, for graciously supplying additional data for this review.
References
Footnotes
PL and TY contributed equally.
Handling editor Jackie A Cassell
Contributors PL and HZ conceived the research topic and study design. PL, TY and HZ designed the protocol and conducted study selection, quality assessment and data extraction. PL contributed to statistical analysis. PL, TY and TF interpreted data. PL, TY, TF and HZ wrote the draft of the manuscript. All authors met ICMJE criteria. All authors contributed to the writing of the manuscript and have seen and approved the final version submitted for publication.
Funding This work was funded by National Natural Science Foundation of China (81703278, 71603166, 81573211, 71673187), National Science and Technology Major Project of China (2018ZX10721102), Australian National Health and Medical Research Council Early Career Fellowship (APP1092621), Sanming Project of Medicine in Shenzhen, China (SZSM201811071), Doris Duke International Clinical Research Fellowship, USA, Medical Research Project Chongqing (2017ZDXM001) and Joint-Innovation Program in Healthcare for Special Scientific Research Projects of Guangzhou, China (201803040002).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.