Article Text

Abstract
Objective Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG) infections can clear without treatment. Despite high prevalence of anorectal infections in men who have sex with men (MSM) and women, studies on anorectal clearance are scarce. Moreover it is unknown whether bacterial load affects urogenital/anorectal CT clearance. In this prospective cohort study, CT and NG clearance is assessed at three anatomical sites of men and women.
Methods CT-positive and NG-positive MSM, heterosexual men and women ≥18 years of age visiting our STI clinic between 2011 and 2013 underwent a repeat test when returning for treatment (n=482). The primary outcome was clearance, defined as a positive nucleic acid amplification test (NAAT) at screening-consultation, followed by a negative NAAT at treatment-consultation. Sociodemographics, sexual risk behaviour and CT bacterial load (inhouse quantitative PCR) were tested as determinants for clearance using multivariable logistic regression for CT and Fisher’s exact test for NG.
Results CT clearance was 9.1% (10/110) for urine, 6.8% (20/292) for vaginal swabs, 12.7% (8/63) for anorectal swabs (ie, 4.0% [1/25] in MSM and 18.4% [7/38] in women) and 57.1% (4/7) for oropharyngeal swabs. For NG this was 33.3% (2/6), 28.6% (2/7), 20.0% (2/10) and 27.3% (6/22), respectively. The number of days between tests (median 10, IQR 7–14) was not associated with clearance. Lower bacterial load at screening was the only predictor for CT clearance (urine mean 1.2 vs 2.6 log CT/mL, p=0.001; vaginal swabs mean 2.1 vs 5.2 log CT/mL p<0.0001; anorectal swabs mean 2.0 vs 3.7 log CT/mL, p=0.002). None of the tested determinants were associated with NG clearance.
Conclusions This study reports the largest number of anorectal infections tested for CT and NG clearance to date. Clearance in all sample types was substantial: between 7% and 57% for CT, and between 20% and 33% for NG (notwithstanding low absolute numbers). CT clearance was associated with a lower load at screening. However, not all individuals with low bacterial CT load cleared the infection, hampering STI guideline change.
- Chlamydia trachomatis
- Neisseria gonorrhoeae
- clearance
- resolution
- natural course
Statistics from Altmetric.com
Introduction
Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG) are the most frequently reported bacterial STI worldwide which can both cause urogenital, anorectal and oropharyngeal infections.1 2 The control of sexually transmitted CT and NG infections continues to challenge many countries.1 Urogenital infections could lead to reproductive tract sequelae in women if left untreated, and infections from other anatomical sites may provide a part in the chain of transmission.3 However, some CT and NG infections may clear without treatment.4–9 Only a few earlier prospective studies were published reporting urogenital CT clearance between 19% and 54% within 1 year using nucleic acid amplification test (NAAT)9–11 and 28% within 3 months using culture.12 For NG, 12.5% (2/16) of young women spontaneously cleared their vaginal NG infection within a maximum follow-up time of 6 weeks.5 It is an ethical challenge to study the natural history of these STIs in humans, as it is not justified to withhold treatment after a CT or NG infection is diagnosed.13 Therefore, most studies used the natural interval between screening and treatment, not withholding a patient’s treatment, reporting urogenital CT clearance between 11% and 44%.7–9 14 15 Despite the high prevalence of anorectal CT infections in men who have sex with men (MSM) and women,3 16–18 previous clearance studies almost exclusively focused on urogenital CT. Only one study assessed anorectal clearance, reporting 18.2% (2/11) CT clearance and 0% (0/6) NG clearance, but absolute numbers were low.19 One study found oropharyngeal CT clearance about one-third in women and MSM.6 Studies on urogenital and oropharyngeal NG clearance between testing and treatment are scarce,4 5 and these are lacking for anorectal NG. Bacterial load could provide insight into the natural course of CT and NG. Previous studies reported that bacterial CT load is mostly stable or decreasing between screening and treatment.6 20 Low bacterial load was associated with oropharyngeal CT clearance.6 However, it is yet unknown whether bacterial load at the time of screening is associated with CT and NG clearance in anogenital samples.
Insight into CT and NG clearance at three anatomical sites could inform parameterisation of the duration of infection, which would be valuable for both clinicians and researchers, and it might inform optimisation of guidelines. In this prospective cohort study, we evaluate CT and NG clearance at the urogenital, anorectal and oropharyngeal sites in men and women visiting the STI clinic, and their associations with various risk factors including recent antibiotic use and bacterial load.
Methods
Study population
This prospective cohort study was carried out between June 2011 and December 2013 at the STI clinic in South Limburg, The Netherlands. Clients who received presumptive treatment, that is, men presenting with urethritis-related symptoms and patients notified by their steady partner, were not eligible for the study (~6%). All untreated CT or NG positives who attended one of five trained study nurses were asked to take a repeat test when returning for treatment (n=509). Exclusion criteria included age below 18 years (n=18 excluded), no test result available (n=4 excluded) and a T1–T2 interval <3 days and >35 days (n=5 excluded). This resulted in 482 paired samples by 469 individuals for analyses; this was 15.8% (482/3050) of all the CT and NG positives during the study period. Each consultation (T1 and T2) included the taking of an electronically registered standardised medical and sexual history. In 12.3% (n=59) of the study population, the T2 questionnaires were missing.
Study procedures
At T1, all participants were tested at the urogenital site and a subset was also tested at the anorectal and/or oropharyngeal site, based on risk group (MSM, swingers, commercial sex workers) or behaviour (self-reported anal sex [receptive or insertive for men] and/or symptoms). At T2, all patients were tested at the same anatomical sites using the same diagnostic test as T1. Specimens were processed at two regional laboratories using different NAATs (strand displacement amplification, Becton Dickinson ProbeTec ET; and PCR, Roche Cobas Amplicor, until 2012, and later Roche Cobas 4800). All NG-positive samples tested by the Roche Cobas Amplicor were confirmed by an inhouse PCR to exclude cross-reactivity with commensal Neisseria spp. All other tests were not confirmed by a second assay. Each of the two laboratories performed about half of all tests included in our study, independent of risk group, anatomical site tested, or day and month of screening. CT and NG clearance was comparable between the two laboratories (results not shown). Serum was tested for syphilis (Treponema pallidum hemagglutination) and HIV in MSM and in women aged 25 and older, according to the Dutch national STI testing guidelines.21
Load quantification
CT load quantification was performed for 380 (79.1%) T1 and T2 samples by an inhouse quantitative PCR (qPCR) as described by Dirks et al .20 In short, TaqMan real-time PCR was used to quantify chlamydial OmpA gene copies/mL. Load values were log-transformed for analyses. Human cell load was assessed in CT-negative and NG-negative samples at T2 to rule out inadequate sampling (n=2 pairs).20 Oropharyngeal CT load (n=7) was not quantified in this study due to the small number of samples and generally low bacterial load.6 The diagnostic NAAT uses a multicopy target (CT plasmid present at 7–10 copies/bacterium), while the inhouse qPCR used for load quantification has a single-copy target (OmpA gene). Therefore, the sensitivity of the load test is lower compared with the diagnostic NAAT, and diagnostic NAAT positive samples can have a load below the quantification limit of the inhouse qPCR.
NG cycle quantification (Cq) values were measured using a different assay that targets a direct repeat region called DR-9 that is specific for NG. The Cobas NAAT uses two sets of primers and probes to detect two highly conserved variations within the DR-9 region. Bacterial loads can be quantified by interpolation of a standard curve of known concentrations of NG. For quantification, a standard curve was made for each specimen type. As the load is derived from the NAAT used for diagnostics, all NG load values were quantifiable.
Statistical analyses
The primary outcome was CT and NG clearance, defined as a positive diagnostic NAAT at T1 followed by a negative diagnostic NAAT at T2 at the same anatomical location. Univariable and multivariable logistic regression analyses were used to identify determinants associated with CT clearance stratified for sample type. Determinants with p<0.10 in univariable analyses were included in the multivariable model. Determinants tested were age (16–20, 21–25 and ≥26 years, based on tertiles), nationality, number of sex partners in the past 6 months (1, 2, ≥3, based on tertiles), antibiotic use <1 month before T1, ever diagnosed with CT at T1, antibiotic use between T1 and T2, urogenital and anorectal symptoms at T1, urogenital and anorectal symptoms at T2, vaginal and anal sexual intercourse between T1 and T2, condom use between T1 and T2, the number of days between T1 and T2 (continuous), CT coinfection (for NG), NG coinfection (for CT), and CT load (for CT). All behavioural data were self-reported.
For NG, Fisher’s exact test was used to identify univariable dichotomous determinants for clearance. NG load was not tested as a determinant for NG clearance due to an underpowered sample size. χ2 and Fisher’s exact tests were used to compare clearance between the different anatomical sites using urine as a reference category; the results are presented in table 1.
CT and NG clearance at T2 in urine, vaginal swabs, anorectal swabs and oropharyngeal swabs, including sensitivity analyses using different scenarios
Sensitivity analyses included the proportion clearance when excluding (1) participants who used antibiotics between T1 and T2, (2) participants with ≥14 days between T1 and T2, (3) participants with sexual exposure between T1 and T2, and (4) participants with unquantifiable load (<1.18 log CT/mL). Sexual exposure was defined as self-reported sexual intercourse with no or inconsistent condom use. Samples with unquantifiable load at T1 were excluded for sensitivity analyses, and samples with unquantifiable load at T2 were defined as ‘cleared’, irrespective of a CT-positive NAAT result. All statistical tests were performed using IBM SPSS Statistics V.21.0 for Windows.
Results
Study population
The study participants were younger compared with non-participants (median 25 years vs 29 years, p<0.0001) and more often had Western nationality (93.2% vs 89.4%, p=0.01). Women more often participated compared with men (22.4% [n=322] vs 11.4% [n=110] of heterosexual men [p<0.0001] and 7.6% [n=48] of MSM [p<0.0001]).
Characteristics of the study population
The median age of the study participants was 22 years (IQR 21–24 years) and majority had Western nationality (95.4%). The median number of sex partners was 2 (IQR 2–3). Urogenital and anorectal symptoms at T1 were reported by 52.8% (n=237) and 4.2% (n=19) of the CT-infected individuals, respectively, and by 32.4% (n=12) and 8.1% (n=3) of the NG-infected individuals, respectively. Three MSM were TPHA-positive, and one MSM was HIV-positive. Nine (1.9%) individuals had a CT–NG coinfection: four women, four MSM and one heterosexual man. Unprotected vaginal intercourse between T1 and T2 was reported by 37.5% (n=158) of patients, and for unprotected anal intercourse this was 3.6% (n=15). Urogenital and anorectal symptoms at T2 were reported by 43.7% (n=171) and 6.9% (n=27) of the CT-infected individuals, and by 25.7% (n=9) and 17.1% (n=6) of the NG-infected individuals, respectively. The median number of days between T1 and T2 for CT was 10 days (IQR 7–14) for urine, 9 days (IQR 7–14) for vaginal swabs, 8 days (IQR 7–14) for anorectal swabs and 12 days (IQR 7–14) for oropharyngeal swabs. For NG this was 8 days (IQR 7–9) for urine, 9 days (IQR 7–14) for vaginal swabs, 7 days (IQR 5–10) for anorectal swabs and 11 days (IQR 7–17) for oropharyngeal swabs (online supplementary table).
Supplemental material
CT clearance and associated determinants
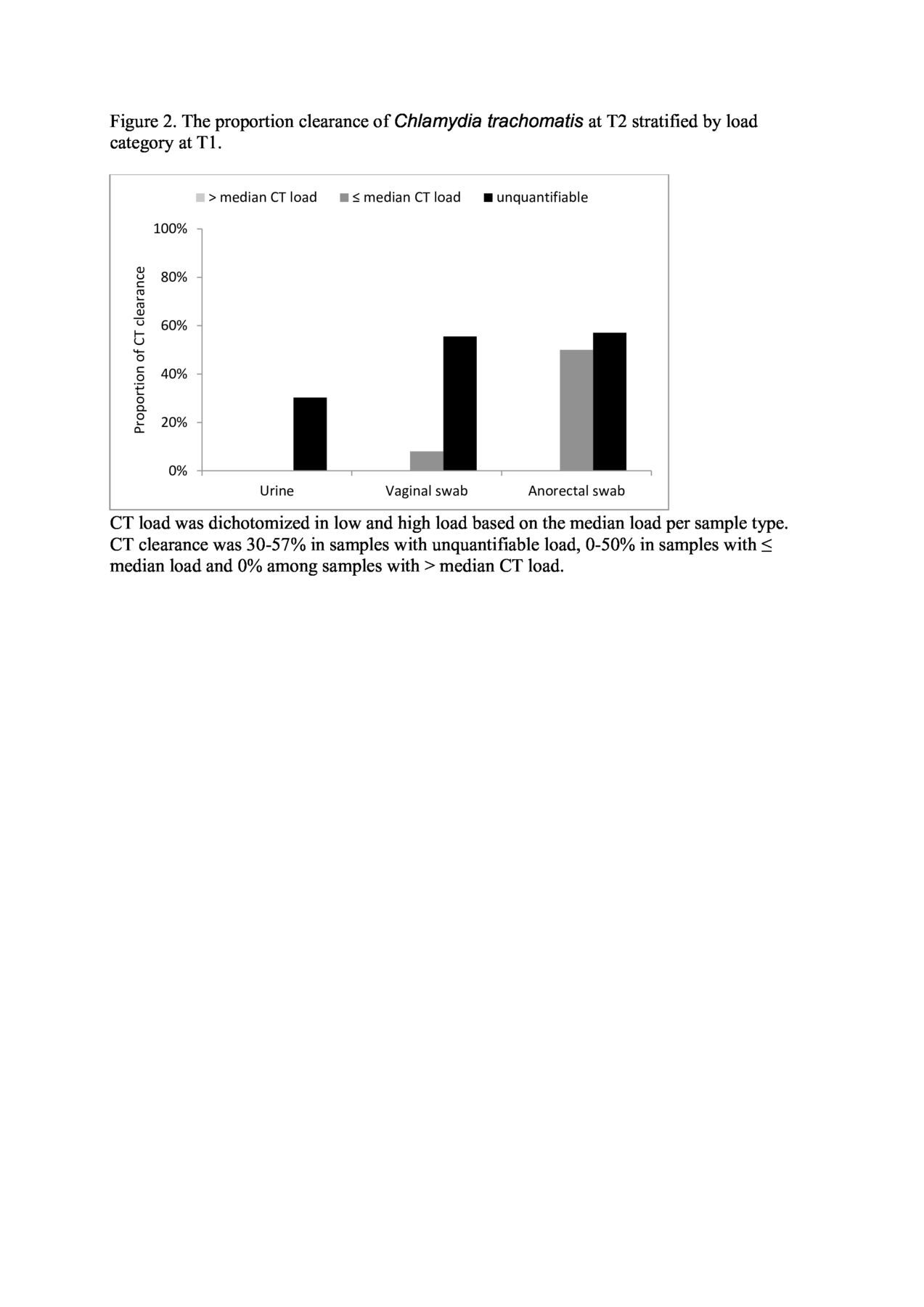
CT clearance in the total population was between 9.1% and 57.1% (table 1). Thirty women had a concurrent genital and anorectal infection at T1, 6.7% (n=2) cleared only the vaginal infection, 10% (n=3) cleared only the anorectal infection and 83.3% (n=25) neither infection. Four MSM had a concurrent genital and anorectal infection and none of the infections cleared. Lower bacterial load was univariately associated with clearance in all sample types. For anorectal swabs in MSM and women, the number of days between T1 and T2 was also univariately associated with clearance (OR 1.23, 95% CI 1.01 to 1.51). Antibiotic use <1 month before T1 and between T1 and T2 was not associated with clearance. Lower chlamydia bacterial load was the only independent determinant in the multivariable analyses for clearance in all sample types (urine OR 11.85, 95% CI 1.52 to 92.37; vaginal swabs OR 3.34, 95% CI 2.18 to 5.12; anorectal swabs OR 9.59, 95% CI 1.95 to 47.12, respectively) (figures 1 and 2). Anorectal CT load was comparable between MSM and women (p=0.78). The sensitivity analyses are presented in table 1.

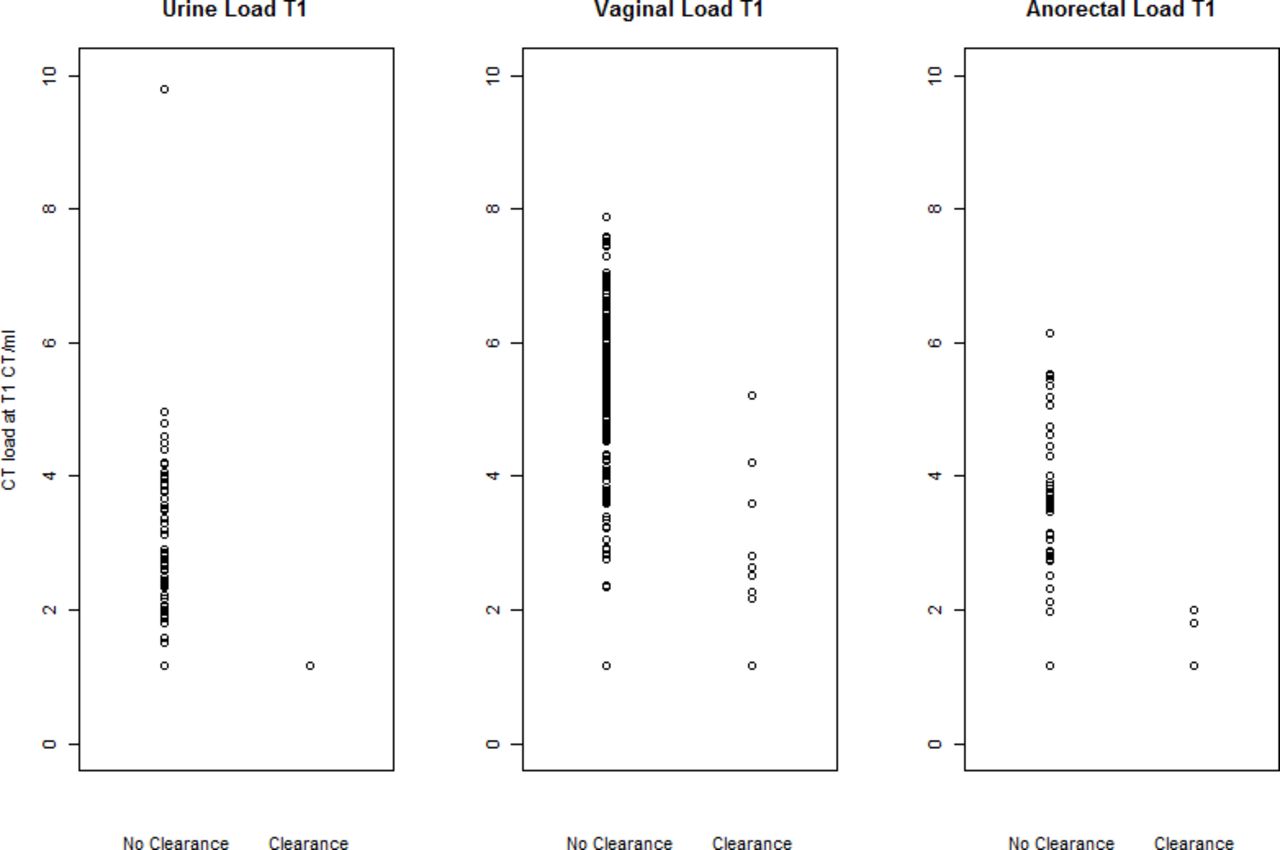
Chlamydia trachomatis (CT) load at T1 stratified by clearance at T2. CT load at T1 was unquantifiable in 33 urine samples (33.7%), 18 vaginal swabs (7.7%) and 6 anorectal swabs (13.0%). CT load at T2 was unquantifiable in 39 urine samples (36.8%), 31 vaginal swabs (12.8%) and 23 anorectal swabs (41.8%). Unquantifiable load in both the T1 and T2 samples was present in 21 urine samples, 13 vaginal samples and 5 anorectal samples. All CT loads are presented in the figure, including the unquantifiable loads. The horizontal line represents the load detection limit.
{kind=link}
{kind=link}
The proportion of clearance of Chlamydia trachomatis (CT) at T2 stratified by load category at T1. CT load was dichotomised in low and high load based on the median load per sample type. CT clearance was 30%–57% in samples with unquantifiable load, 0%–50% in samples with less than or equal to the median load and 0% among samples with greater than the median CT load.
NG clearance and associated determinants
NG clearance in the total population was between 20% and 33% (table 1). One woman had concurrent NG at all three anatomical sites, and none of the infections cleared. Two MSM had concurrent NG at all three anatomical sites, one cleared all sites and one cleared all sites except the oropharyngeal site. Two MSM with concurrent anorectal and oropharyngeal NG did not clear any infection. None of the tested determinants were associated with NG clearance in any of the sample types. NG load is presented in table 2.
Log10 transformed NG bacterial load per millilitre at T1 and T2 in urine, vaginal swabs, anorectal swabs and oropharyngeal swabs, stratified by clearance at T2
Discussion
In this prospective study, we evaluate for the first time CT and NG clearance at all three anatomical sites in both men and women. This study reports the largest number of CT and NG anorectal infections tested for clearance to date. CT clearance was 7%–57% between screening and treatment with a median of 10 days. For NG this was between 20% and 33%, although absolute numbers were low.
Anorectal infections are at least as prevalent as urogenital infections in MSM and women.3 22 The only previous study by Apewokin et al reported 18% (2/11) anorectal CT clearance and 0% (0/4) anorectal NG clearance with a median of 11 days.19 This is comparable with our study for CT (4%–18%), although the study population was different from ours in HIV positivity at 0.1% vs 48% in the other study. This might have influenced clearance.
In concordance with previous studies, oropharyngeal CT clearance between screening and treatment was found to be higher (36%–57%)6 19 compared with urogenital clearance (11%–44%).7–9 14 15 19 This could be due to an overall lower load in oropharyngeal samples.6 23 A larger study from the Netherlands including 1266 cases reported only 11% oropharyngeal NG clearance4 vs 27% in our study. This difference could be due to different NAATs or different cut-off values, which cause preselection for higher loads at T1 and thereby lower clearance rates, although lower absolute numbers and a large CI should be taken into account when interpreting the results of our study.
A wide range of determinants were tested for association with CT and NG clearance, such as antibiotic use and possible reinfection by sexual exposure. Some previous studies report on the association between a prior CT infection and protective immunity7 15 24 or with older age as a proxy for prior infection.12 In this study, older age and prior CT infection were both not associated with clearance, as in a study by Geisler et al from 2008,8 indicating an ongoing debate.13
Lower CT load at the time of screening was the only independently associated determinant for subsequent CT clearance in all sample types in our study. Clearance rates were highest in lower load categories, especially for urine in which all cleared samples had unquantifiable load. For example, in the highest load category, that is, above the median load, clearance rates were 0% in all sample types, indicating infections with viable replicating bacteria. Not all individuals with a low load cleared the infection. Therefore, the impact of these results on STI testing guidelines, policy and practice is limited. Although qualitative PCR results are not yet widely used in clinical care, real-time qPCR is the standard commercially available test, making cycle threshold or Cq values available as a proxy for bacterial load. This makes clinical decisions based on these values within the reach of daily practice.
None of the tested determinants were associated with NG clearance in any of the sample types. A study from the USA found that vaginal NG load did not seem to be associated with duration of infection after follow-up of 12 weeks.5
Due to the symptomatic nature of NG infections, the low number of included NG infections could be due to presumptive blind treatment at initial consultation (T1). NG clearance rates could be overestimated, as probably more asymptomatic infections with lower load were included in this study.
A general limitation of clearance and natural history studies is that the time of infection is unknown; this could influence antibody production by the host immune system and thereby the bacterial load. Antibody detection could be useful to exclude individuals who were exposed to CT or NG at T1, but who were not infected.25 However, infection cannot be ruled out by the absence of antibodies.
The exact day of clearance is unknown, as we did not collect daily samples. Genotyping was not performed, and clearance rates could differ between OmpA genotypes.26 Genotyping would also be valuable to exclude reinfections by other serovars, as positive NAAT results at T2 were classified as ‘not cleared’ in this study. However, self-report of unprotected intercourse was not associated with clearance.
Our bacterial load assay had a lower sensitivity than our regular diagnostic NAAT, resulting in some samples with unquantifiable load. Sensitivity analyses excluding samples with unquantifiable load revealed higher clearance rates in urine (18.5%) and anorectal swabs (24.4%), and comparable clearance in vaginal swabs (6.4%). Possibly, using a single sensitive diagnostic NAAT to assess clearance could have resulted in detecting false positives or false negatives.27 On–off effects, that is, a positive and a negative test result in the same sample, might occur in samples with a low bacterial load around the detection limit, although evidence for this effect is limited. Viability testing could provide more insight into the clinical significance of test positivity by identifying individuals with viable chlamydia bacteria, that is, biologically plausible for transmission and complications, versus exposed individuals without viable chlamydia bacteria, for whom the risk for transmission and complications is unknown.28 29
We cannot entirely rule out contamination of swabs by sampling, for example contamination of an anorectal swab with vaginal secretions during sampling, despite clear written and visual instructions. However, it is unlikely that contamination of the swabs would explain the proportion of clearance we found in this study. Too few data on recent sexual exposure prior to T1 were available, and therefore not included in the analyses. Study inclusion was moderate (16%), due to limited study nurse capacity. Study participation was estimated at 90%, based on the study nurse feedback as study refusal was not systematically recorded. Participants were more often young, Western and women compared with the non-participants. However, these characteristics were not associated with the biomedical phenomenon of clearance, and we believe this does not have an impact on the internal validity of the study.
In conclusion, this is the first study to assess both CT and NG clearance at three anatomical sites in MSM, heterosexual men and women. Between 7% and 57% of the CT infections and between 20% and 33% of NG infections cleared between screening and treatment. This indicates that screening and treatment remain important to limit transmission in the population. Lower CT load at the time of screening was the only independent determinant for CT clearance in all sample types. Not all individuals with low bacterial CT load cleared the infection, hampering STI guideline change.
Key messages
Although anorectal Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG) (for men who have sex with men [MSM]) infections are common in MSM and women, clearance studies for anorectal infections are scarce.
Clearance between screening and treatment was substantial in all sample types: between 7% and 57% for CT, and between 20% and 33% for NG (notwithstanding low absolute numbers).
Lower bacterial CT load at the time of screening was the only independent predictor for CT clearance in all sample types.
Not all individuals with low bacterial CT load cleared the infection, hampering STI guideline change.
Acknowledgments
The authors thank the staff of the STI clinic, South Limburg for their valuable contribution to the sample collection, especially Ms Eslie Bos for coordinating the study at the STI clinic. Furthermore we would like to thank Mr Brian van der Veer for providing the NG cycle quantification values.
References
Footnotes
Handling editor Jackie A Cassell
Contributors NHTMD-M and CJPAH designed the study. GAFSvL was involved in planning and supervision of the study. JAMCD performed laboratory analyses under the supervision of PW. GAFSvL performed statistical analyses under the supervision of NHTMD-M. GAFSvL wrote the first version of the manuscript, and all authors contributed to the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Medical Ethical Committee of Maastricht University approved the study (10-4-066). All study participants provided written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.