Article Text

Abstract
Background Genital chlamydia infection in women is often asymptomatic, but may result in adverse outcomes before and during pregnancy. The purpose of this study was to examine the strength of the relationships between chlamydia infection and different reproductive health outcomes and to assess the certainty of the evidence.
Methods This review was registered and followed the Cochrane guidelines. We searched three databases to quantitatively examine adverse outcomes associated with chlamydia infection. We included pregnancy and fertility-related outcomes. We performed meta-analyses on different study designs for various adverse outcomes using unadjusted and adjusted analyses.
Results We identified 4730 unique citations and included 107 studies reporting 12 pregnancy and fertility-related outcomes. Sixty-eight studies were conducted in high-income countries, 37 studies were conducted in low-income or middle-income countries, and 2 studies were conducted in both high-income and low-income countries. Chlamydia infection was positively associated with almost all of the 12 included pregnancy and fertility-related adverse outcomes in unadjusted analyses, including stillbirth (OR=5.05, 95% CI 2.95 to 8.65 for case–control studies and risk ratio=1.28, 95% CI 1.09 to 1.51 for cohort studies) and spontaneous abortion (OR=1.30, 95% CI 1.14 to 1.49 for case–control studies and risk ratio=1.47, 95% CI 1.16 to 1.85 for cohort studies). However, there were biases in the design and conduct of individual studies, affecting the certainty of the overall body of evidence. The risk of adverse outcomes associated with chlamydia is higher in low-income and middle-income countries compared with high-income countries.
Conclusion Chlamydia is associated with an increased risk of several pregnancy and fertility-related adverse outcomes in unadjusted analyses, especially in low-income and middle-income countries. Further research on how to prevent the sequelae of chlamydia in pregnant women is needed.
Trial registration number CRD42017056818.
- chlamydia trachomatis
- pregnancy
- infertility
- meta-analysis
- women
Statistics from Altmetric.com
Background
Chlamydia trachomatis is the most common bacterial STI in the world.1–3 In 2012, the global prevalence of chlamydia infection was 4.2% in women.4 Untreated chlamydia infection can cause pelvic inflammatory disease, mucopurulent cervicitis and endometritis.5–7 Chlamydia infection has been linked to spontaneous abortion, chorioamnionitis, preterm premature rupture of membranes, ectopic pregnancy, premature delivery and stillbirth.8–10 In addition, chlamydia increases the risk of male and female infertility. Understanding the strength of associations between chlamydia infection and adverse outcomes before and during pregnancy is essential for improving maternal and child health programmes.
Guidelines on chlamydia screening during pregnancy vary widely. The WHO recommends a syndromic approach, which has been shown to miss 20%–70% of cases.11 While US Centers for Disease Control and Prevention guidelines advocate for universal chlamydia screening in pregnant women,12 UK guidelines do not recommend routine chlamydia screening in pregnant women.13 There are limited data on the cost-effectiveness of prenatal chlamydia screening and treatment programmes.14 Modelling studies suggest that the effectiveness of chlamydia screening largely depends on the likelihood of developing adverse outcomes.15–17
To better inform modelling studies and policy, more evidence is needed examining the associations between chlamydia infection and adverse pregnancy outcomes. Previous studies estimating the global burden of chlamydia infection18 19 suggested the cost-effectiveness of chlamydia screening among women20 and identified morbidity associated with chlamydia infection in pregnancy as a significant global health problem, especially in low-income and middle-income countries.11 21 In addition, a few studies have confirmed the association between chlamydia infection and pregnancy and fertility-related adverse outcomes.22 23 However, limited studies have evaluated the bias in the design and conduct of individual studies that investigated these associations, and almost no study has summarised the certainty of the overall body of evidence. The purpose of our study was to examine the strength of the relationships between chlamydia infection and different reproductive health outcomes and to assess the certainty of the evidence.
Methods
The protocol for this study was registered in PROSPERO, the International Prospective Register of Systematic Reviews (see online supplementary 1 for study protocol). We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist in writing and reporting this systematic review (online supplementary data 2).24
Supplemental material
Search strategy and selection criteria
We searched three electronic databases (Medline via PubMed, EMBASE and Cochrane) for studies on the relationship between chlamydia infection and any adverse outcomes related to pregnancy. The search terms are provided in online supplementary data 3.
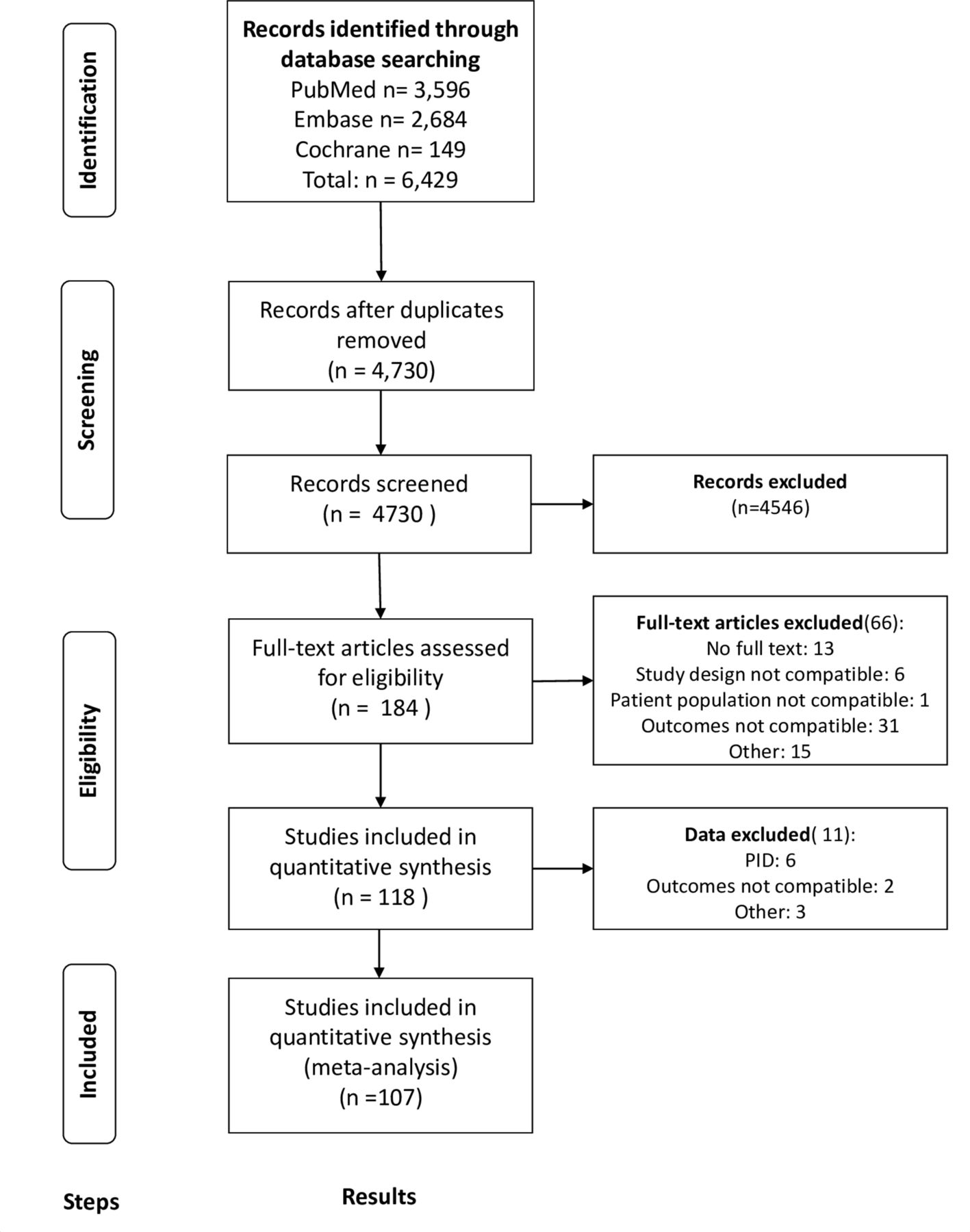
We included studies published in English before 31 May 2018 if they were quantitative and published in a peer-reviewed journal, including randomised controlled trials, prospective cohorts, retrospective cohorts, case–control studies and cross-sectional studies. We excluded dissertations, conference abstracts, non-English-language publications and studies that did not quantitatively report data on adverse outcomes. Two independent reviewers (JM and WT) evaluated titles and abstracts for relevance. Full-text articles were gathered with the assistance of a global health librarian experienced in search algorithm development. Each full-text article was also assessed by two of four independent reviewers (JM, WT, RF or WC). Discrepancies were brought to a third independent reviewer (JDT) for discussion and resolution. We did not obtain original data sets from authors. Detailed study screening methods and a PRISMA flow diagram are provided in figure 1.

PRISMA flow chart. PID, pelvic inflammatory disease; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
We extracted the following variables for each publication: author, journal, year, study design, study period, population demographics, sample size, study country, chlamydia diagnostic, history of chlamydia treatment, HIV infection and adverse pregnancy outcomes. For case–control studies and cross-sectional studies, we extracted the numbers of patients with and without chlamydia infection among cases (women with adverse pregnancy outcomes) and among controls (women without adverse pregnancy outcomes). For cohort studies, we extracted cases and non-cases in the exposed group (women with chlamydia infection) and the unexposed group (women without chlamydia infection). In addition, we extracted the adjusted OR or risk ratio (RR) from the included studies, if reported. We defined study as a single publication which may include multiple findings relevant to several study results.
Assessment of risk of bias and study quality
For each study, we assessed the risk of bias using the Quality Assessment Tool for Quantitative Studies.25 26 Two reviewers assessed the risk of bias in six categories: selection bias, study design, confounders, blinding, data collection methods, withdrawals and dropouts. Each component was given a rating of 1 (strong quality) to 3 (weak quality).26 The risk of bias in each study is reported in online supplementary data 4A. We then assessed the certainty of the evidence for each outcome using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) working group criteria.27 The summary of the findings and the level of certainty of the overall body of evidence were assessed using GRADEpro V.3.6 for Windows. Definitions for the included adverse outcomes are provided in the GRADE table (online supplementary data 6). We compared findings from higher quality and lower quality studies with the overall quality based on an assessment of the flaws in different domains and the seriousness of the flaws.
Analysis and synthesis
We examined a total of nine pregnancy-related adverse outcomes: stillbirth, infant death, spontaneous abortion, preterm labour (<37 weeks), low birth weight, small for gestational age, premature rupture of membranes, postpartum endometritis and pre-eclampsia. We examined three fertility-related outcomes: infertility, tubal factor infertility and ectopic pregnancy. Tubal factor infertility was defined in women having proven infertility due to tubal occlusion (bilateral or unilateral) and confirmed by laparoscopy. For each case–control study and cross-sectional study, we calculated ORs from raw published study data. For each cohort study, we calculated relative effects from raw published study data. For the included studies, we included all women diagnosed with chlamydia as cases or exposures regardless of whether they were treated. For infertility, we included tubal factor infertility as a subgroup. We also extracted the adjusted estimates available in the literature and compared them with the unadjusted estimates. A Z-test was used to compare the log-transformed pooled crude estimates and the pooled adjusted estimates.
We conducted 37 meta-analyses to determine the pooled OR or RR of chlamydia in women with adverse outcomes compared with women without chlamydia (table 1). Meta-analyses were done according to outcomes and study designs. As there were limited studies with adjusted outcomes, we reported unadjusted relative effect in the forest plots. Meta-analyses were performed using STATA V.15.0. Heterogeneity was assessed with an I2 statistic.28 We used a random-effects model. In comparison with a fixed-effects model, a random-effects model has a wider CI for the underlying parameter and better anticipates the possibility that other unpublished studies may report different outcomes from those included in the meta-analysis.29 To detect publication bias, we visually inspected funnel plots for asymmetry for each meta-analysis with 10 or more studies. An Egger test was also used to detect publication bias.
Summary of findings for quantitative analysis from the case–control and cohort studies, with unadjusted and adjusted results
To investigate potential causes of heterogeneity, we conducted subgroup analyses among all outcomes with 10 or more case–control studies based on World Bank income classification (high-income vs low-middle-income countries), year of publication (before or after 2000) and category of specimen type as a surrogate for diagnostic accuracy (serum vs urine or reproductive tract). If a study could not be classified into either subgroup, we excluded it from the subgroup analysis. Adjusted RRs were used in subgroup analyses.
Results
Study selection
A total of 6429 studies were identified and 1699 duplicates were removed. Each of the 4730 unique titles was examined and 4506 studies were excluded. The resulting 224 full-text studies were examined and 117 of these were excluded: 104 full-text articles did not meet inclusion criteria, and the full texts for 13 studies were unable to be located. A total of 107 studies reporting a total of 160 observations were included in the analysis. We focused on reporting 12 study outcomes (figure 1, online supplementary data 4B).
Of the 107 included studies, 36 studies analysed more than one outcome. Thirty-seven studies were conducted in low-middle-income countries and 68 were conducted in high-income countries. Two studies were conducted in both low-middle-income and high-income countries. Forty-eight studies were conducted before 2000, and 59 studies were conducted in 2000 or later (online supplementary data 4B). All studies included in this review were case–control studies, cross-sectional studies or cohort studies. Only two studies specified whether patients received treatment for chlamydia. The sample size for the included studies ranged from 55 to 354 127, with a median of 326 participants. Diagnostic methods varied widely across studies. Fifty-six studies used serum samples for diagnosis, and 51 studies used urine or reproductive tract samples.
All included studies investigated the relationship between chlamydia and adverse pregnancy outcomes (see online supplementary data 4B). Among the 107 included studies, they examined the impact of chlamydia on stillbirth (7 studies),30–36 infant death (3 studies),37–39 infertility (30 studies)5 40–60 w1–w8 (see online supplementary data 11), tubal factor infertility (12 studies),5 41 42 44 48 50 54 57 58 w1 w3 w5 spontaneous abortion (23 studies),59 60 w2 w6 w9–w25 preterm birth (25 studies),31 32 34 35 37 78 w24 w26–w44 ectopic pregnancy (29 studies),5 30 45 48 w5 w8 w15 w18 w45–w65 low birth weight (11 studies),34 37 38 w24 w26 w30 w32 w34 w36 w43 w66 small for gestational age (6 studies),32 34 35 38 w39 w66 premature rupture of membranes (8 studies),34 37 w23 w32 w42 w67–w69 postpartum endometritis (4 studies)34 w30 w70 w71 and pre-eclampsia (2 studies).w72 w73 Nine studies contained outcomes for both tubal infertility and infertility. As a result, we stratified the results within each of the nine studies and provided separate effect estimates. We conducted a total of 37 meta-analyses, including one for each outcome for each study design. This included 34 for case–control and cohort studies (table 1) and 3 for cross-sectional studies (online supplementary data 7). All included studies for each of these meta-analyses are listed in online supplementary data 4B.
Risk of bias in individual studies and overall certainty of the evidence
We examined the risk of bias in individual studies based on the six domains. The overall risk of bias analysis suggests that the original quality of the included studies is low. These findings are presented in online supplementary data 4A.
We examined biases associated with small studies. In order to assess biases associated with small studies, we examined funnel plots for case–control studies of infertility, case–control studies of spontaneous abortion, case–control studies of preterm birth, cohort studies of preterm birth and case–control studies of ectopic pregnancy (online supplementary data 5). Most of the funnel plots were roughly symmetrical except for case–control studies of preterm birth (bias (95% CI)=2.67 (0.39 to 4.95), p=0.027) and case–control studies of spontaneous abortion (bias (95% CI)=3.00 (0.70 to 5.31), p=0.015). In these two funnel plots, the gap in the lower left of the funnel suggests that studies with low precision and small ORs have not been published.
We examined the overall certainty associated with the evidence. The overall certainty for each of the 12 pregnancy and fertility-related adverse outcomes was either low or very low (table 1). These results are further detailed in online supplementary data 6. We also present the results for each relevant outcome from cross-sectional studies in online supplementary data 7. However, we could not obtain adjusted ORs for cross-sectional studies because of the small number of cross-sectional studies and the fact that few controlled for confounders.
online supplementary data 8 shows forest plots for the three meta-analyses related to stillbirth, spontaneous abortion and infertility in some, but not all study designs. The ORs reported in online supplementary data 8 are only from case–control studies.
For stillbirth, in the meta-analyses of case–control studies, the odds of chlamydia were higher among women with stillbirth than women without stillbirth (pooled unadjusted OR=5.05, 95% CI 2.95 to 8.65, I2=33.7%, n=610; online supplementary data 8). In the meta-analysis of cohort studies, the RR of stillbirth was higher among women with chlamydia than women without chlamydia (pooled unadjusted RR=1.28, 95% CI 1.09 to 1.51, I2=19%, n=415 094; online supplementary data 8).
For spontaneous abortion, the odds of chlamydia infection in case–control studies were higher among women with spontaneous abortion compared with women without spontaneous abortion (pooled unadjusted OR=1.30, 95% CI 1.14 to 1.49, I2=81.1%, n=11 694; online supplementary data 8). The RR of spontaneous abortion in cohort studies was higher among women with chlamydia compared with women without chlamydia (pooled unadjusted RR=1.47, 95% CI 1.16 to 1.85, I2=50.6%, n=1592).
For infertility, the odds of chlamydia in case–control studies were higher among women with infertility compared with women without infertility (pooled unadjusted OR=2.72, 95% CI 2.37 to 3.12, I2=82.7%, n=8049; online supplementary data 8). The RR of infertility in cohort studies was higher among women with chlamydia compared with women without chlamydia (pooled unadjusted RR=1.84, 95% CI 1.77 to 1.90, I2=90.9%, n=573 250).
Our meta-analysis also suggests that chlamydia is associated with infant death (unadjusted OR=1.86, 95% CI 1.12 to 3.10, I2=0%; unadjusted RR=1.87, 95% CI 0.76 to 4.56, I2=not available), preterm labour (unadjusted OR=1.29, 95% CI 1.11 to 1.50, I2=81.7%; unadjusted RR=1.54, 95% CI 1.48 to 1.60, I2 =98%), ectopic pregnancy (unadjusted OR=3.24, 95% CI 2.95 to 3.55, I2=87.0%; unadjusted RR=1.67, 95% CI 1.64 to 1.70, I2 =89.4%), low birth weight (unadjusted OR=1.80, 95% CI 1.20 to 2.71, I2=61.1%; unadjusted RR=1.33, 95% CI 1.27 to 1.40, I2 =49%) and premature rupture of membranes (unadjusted OR=2.34, 95% CI 1.19 to 4.60, I2=0%; unadjusted RR=1.53, 95% CI 1.20 to 1.96, I2 =51.3%). We also observed an association between chlamydia and small for gestational age in case–control studies (unadjusted OR=1.64, 95% CI 0.81 to 3.31, I2=59%) and cohort studies (unadjusted RR=1.19, 95% CI 1.13 to 1.29, I2 =0%). In cohort studies, we also observed an association between chlamydia and postpartum endometritis (unadjusted RR=1.61, 95% CI 1.24 to 2.08, I2 =58.9%). Forest plots for these outcomes are provided in online supplementary data 9. For both case–control and cohort studies, 6 out of 11 meta-analyses of these study designs had I2 >50%. The overall certainty of evidence associating with each of these findings is presented in online supplementary data 6.
Comparison of unadjusted ORs with adjusted ORs
Within each study design, we compared the pooled unadjusted estimates with the pooled adjusted estimates. Results showed that the point estimate is lower for the adjusted estimate compared with the unadjusted estimate for several outcomes (spontaneous abortion, infertility, tubal infertility, stillbirth, infant death, preterm labour), suggesting that controlling for confounding reduces the strength of association (table 1).
Subgroup meta-analyses
We also conducted subgroup meta-analyses on case–control studies by country income level (low vs middle or high), year of publication (before or after 2000) and diagnostic sample (serum vs reproductive tract or urine) for spontaneous abortion, preterm labour, low birth weight, infertility, tubal factor infertility and ectopic pregnancy (online supplementary data 10). We did not conduct subgroup meta-analyses for cohort studies because most cohort studies were conducted in high-income countries, implemented after 2000 and used serum testing. We did not include low birth weight in the subgroup analyses because there were insufficient data for the subgroups of low-income countries, before 2000 and serum testing. We did not include tubal factor infertility in the subgroup analyses by diagnostic sample because there were insufficient data from a reproductive tract sample.
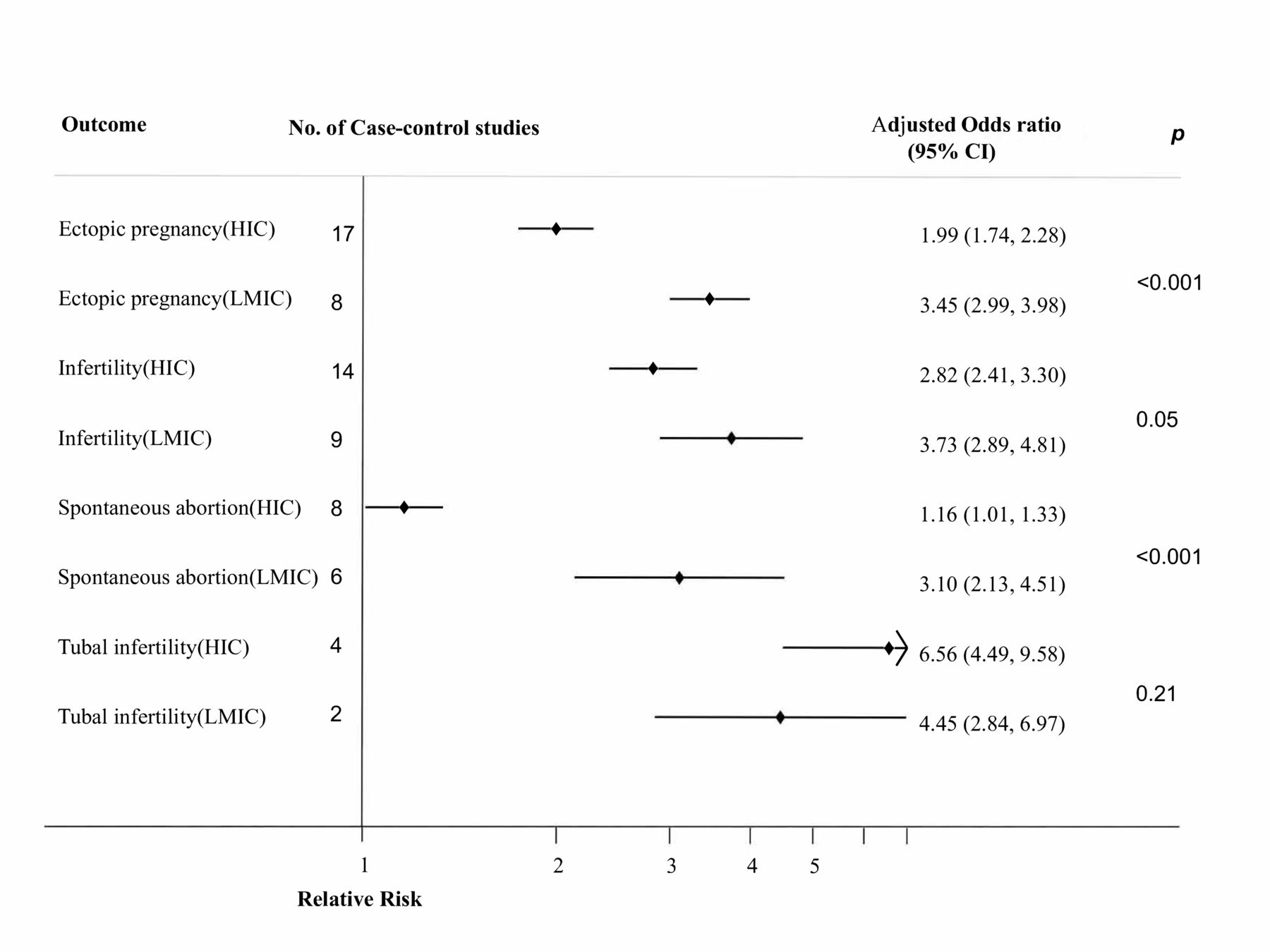
The association of spontaneous abortion with chlamydia was higher in low-middle-income countries (adjusted OR=3.10, 95% CI 2.13 to 4.52, I2=79.3%, n=1287) than in high-income countries (adjusted OR=1.16, 95% CI 1.01 to 1.51, I2=62.7%, n=10 407, p<0.001). We identified two studies that reported an adjusted association between spontaneous abortion and chlamydia infection in high-income countries (adjusted OR=0.97, 95% CI 0.79 to 1.19, I2=0%, n=2858). The association of infertility with chlamydia infection was higher in low-middle-income countries (adjusted OR=3.73, 95% CI 2.89 to 4.82, I2=82.2%, n=1854) compared with high-income countries (adjusted OR=2.82, 95% CI 2.41 to 3.31, I2=86.1%, n=5496, p=0.07). However, the association of tubal factor infertility with chlamydia infection was lower in low-middle-income countries (adjusted OR=4.45, 95% CI 2.84 to 6.99, I2=96%, n=412) compared with high-income countries (adjusted OR=6.56, 95% CI 4.49 to 9.58, I2=62.1%, n=761). For ectopic pregnancy, the association with chlamydia was stronger in low-middle-income countries (adjusted OR=3.45, 95% CI 2.99 to 3.98, I2=73, n=3791) compared with high-income countries (adjusted OR=1.99, 95% CI 1.74 to 2.27, I2=62%, n=6997, p<0.001) (figure 2, online supplementary data 10).
{kind=link}
{kind=link}
Subgroup analysis of ectopic pregnancy, infertility, tubal infertility and spontaneous abortion by country income (case–control studies only). HIC, high-income countries; LMIC, low-income and middle-income countries.
We also compared pooled results for spontaneous abortion, preterm labour, low birth weight, infertility, tubal factor infertility and ectopic pregnancy based on study quality. The association between spontaneous abortion and chlamydia was higher in lower quality studies (adjusted OR=1.83, 95% CI 1.50 to 2.23, I2=78.7%, n=16 547) than in higher quality studies (adjusted OR=1.01, 95% CI 0.84 to 1.21, I2=37.6%, n=5147, p<0.001). The association between infertility and chlamydia was higher in lower quality studies (adjusted OR=3.39, 95% CI 2.93 to 3.93, I2=84.6%, n=4676) compared with higher quality studies (adjusted OR=1.60, 95% CI 1.18 to 2.16, I2=87.9%, n=3373, p<0.001). In addition, the association between tubal factor infertility with chlamydia infection was higher in lower quality studies (adjusted OR=4.27, 95% CI 4.18 to 7.47, I2=86.8%, n=1173) than in higher quality studies (adjusted OR=1.20, 95% CI 0.64 to 2.25, n=699, p<0.001) (online supplementary data 10).
Discussion
We conducted a global systematic review and meta-analysis on the association between chlamydia and adverse pregnancy and reproductive health outcomes among women. A previous review examined the prevalence of chlamydia infection in low-middle-income countries.11 Our review extends previous work by quantifying the association between chlamydia and several pregnancy-related outcomes. Our unadjusted analyses suggested that chlamydia is moderately associated with 10 of the 12 adverse pregnancy and reproductive health outcomes.
We found that chlamydia was associated with stillbirth and spontaneous abortion. This finding is consistent with two previous reviews which reported that chlamydia in pregnancy is positively associated with intrauterine fetal demise. However, those two studies did not disaggregate studies conducted in high-income countries and studies conducted in low-middle-income countries.w74 w75 11 w76 Our review included more low-middle-income country studies and more definitively addressed the link between chlamydia and stillbirth. Similarly, spontaneous abortion has not been a well-established adverse outcome of chlamydia infection in pregnancy,w77–w79 in part because causes of spontaneous abortion are difficult to ascertain.8 w78 w80 Our review provided additional evidence for the relationships between chlamydia and these two adverse outcomes.
Our results suggest that chlamydia infection is associated with infertility, especially tubal factor infertility. This is consistent with several studies that examined chlamydia infection and fertility.22 w81 w82 In low-middle-income countries, infertility is a particularly challenging problem due to stigma and the lack of resources available for assisted reproductive technologies.w83 w84 Previous studies have identified bacterial reproductive tract infections as a major contributor to infertility in low-middle-income countries.11 w83 w85
We found that the associations between chlamydia and spontaneous abortion, infertility and ectopic pregnancy were stronger in low-middle-income countries compared with high-income countries. This finding is consistent with previous work showing a higher prevalence and morbidity of chlamydia in low-middle-income countries compared with high-income countries.11 18 Although research from low-middle-income countries was limited, this difference may suggest disparities in the detection and treatment of chlamydia. Previous research has highlighted the challenges of managing STIs in low-middle-income countries.11 w86 Resource-constrained settings may lack funds to procure diagnostics and often must rely on a syndromic approach to clinical management.w86 Furthermore, partner management can be difficult,w87 leading to high rates of reinfection.w88
However, there were biases in the design and conduct of individual studies that investigated causal associations. We found that pooled unadjusted estimates were slightly higher than pooled adjusted estimates. In addition, the pooled estimates in case–control studies were higher than in cohort studies. These findings indicate that the pooled estimates may be subject to bias related to study design and data analysis. When using data on associations to make aetiological inferences, we should take study design and adjustment for confounding into consideration. However, most of the included studies did not report an adjusted result. For example, for spontaneous abortion, only two studies, both from high-income countries, adjusted for confounders.
There are several potential mechanisms by which C. trachomatis could cause pregnancy and fertility-related adverse outcomes: ascending infection to the upper reproductive tract; persistent chlamydia infection; a proinflammatory response in the epithelium to either the bacteria or specific antigens; or cHSP60-induced delayed hypersensitivity.w89 w90 However, these mechanisms were not addressed in the included studies and require further investigation. We also found that observational study design, lack of blinding and no adjustment for confounders contributed to bias. When designing future studies, researchers should take these biases into consideration.
Our review has some limitations. First, we observed substantial heterogeneity across studies, and many included studies only reported unadjusted estimates. This is likely due to differences in study populations and study design. All studies included in this review were observational studies, resulting in their overall quality being classified as low or very low. We acknowledge that the included studies are inevitably at higher risk of bias, especially from confounding variables such as medical history. For example, syphilis is more common among women with chlamydia infection and is also known to cause adverse pregnancy outcomes. Second, studies varied in diagnostic method, and some studies used serological diagnostic methods. Serology may detect a previous rather than current infection.w91 However, our subanalysis did not show a consistent difference between serologically diagnosed chlamydia and chlamydia diagnosed based on urine or reproductive tract samples (online supplementary data 10). Third, 105 out of the 107 included studies did not provide information on previous chlamydia treatment. Some high-income countries have guidelines on screening and resources to implement these guidelines, which likely resulted in a high proportion of chlamydia-infected pregnant women receiving treatment. Studies in which patients were recently treated may cause our analysis to underestimate the strength of the association between chlamydia and adverse outcomes. In addition, the strengths of association were potentially underestimated in high-income countries when compared with low-middle-income countries because treatment coverage may be higher in high-income countries. Fourth, we did not include grey literature and non-English-language publications, which may lead to selection bias. Finally, only a minority of studies came from low-middle-income countries, despite the increased burden of infection in low-middle-income countries.
Conclusion
Our review demonstrates associations between chlamydia and several pregnancy and fertility-related adverse outcomes. These findings suggest a greater association between chlamydia and adverse outcomes in low-middle-income countries compared with high-income countries. Our study further highlights the need for continued health systems strengthening to prevent, screen, diagnose and treat chlamydia infection in pregnant women.
Key messages
Chlamydia trachomatis is associated with many adverse pregnancy and fertility-related outcomes in unadjusted analyses.
However, due to biases in the design and conduct of individual studies, the overall certainty of the evidence was low.
There is a stronger association between chlamydia infection and adverse pregnancy outcomes in low-income and middle-income countries compared with high-income countries.
Further research on how to prevent the sequelae of chlamydia in pregnant women is needed.
Abstract translation
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.Acknowledgments
We would like to acknowledge Xiaojing Zheng of the School of Medicine at the University of North Carolina at Chapel Hill, Dr Kevin Dunbar, Dr Cristina Visintin and Dr John Marshall of Public Health England, and Dr Yang Bin and Dr Zheng Heping from the Southern Medical University Dermatology Hospital for their suggestions and feedback. In particular, we would like to thank Ms Juan Nie for her assistance with the revision of this manuscript.
References
Footnotes
Handling editor Nicola Low
WT, JM and KTL contributed equally.
Contributors JM, WT and JDT drafted the protocol. JSW performed the literature search. JM, WT, WC and RF extracted the data. JDT solved the inconsistency in the data extraction process. RC and WT evaluated the quality of the evidence. JK, TD, RC and JM contributed ideas for analysis. WT and KTL did the statistical analysis and interpreted the results. KTL and WT wrote the manuscript with input from JDT, JK, TD, RC and JM.
Funding This work was supported by the National Institutes of Health [NIAID 1R01AI114310, K24AI143471, and R34MH119963].
Competing interests JK has received research support and donated testing supplies from Cepheid and Hologic.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.