Article Text

Abstract
Objectives Antimicrobial resistance is generally linked to antimicrobial selection pressure. Antimicrobial-resistant Neisseria gonorrhoeae infections frequently emerge in core groups. We hypothesised that these groups are more often exposed to antimicrobials as a consequence of the repeated treatment of both symptomatic and asymptomatic sexually transmitted infections (STIs) and that frequent STI screening in asymptomatic patients may contribute indirectly to antimicrobial exposure. In this study, we explored the ecological association between screening intensity in men who have sex with men and antimicrobial susceptibility in N. gonorrhoeae in the USA.
Methods Data on STI screening intensity came from the American Men’s Internet Survey between October 2014 and March 2015. Data on gonococcal susceptibility to azithromycin, ceftriaxone and cefixime were used from the Gonococcal Isolate Surveillance Project in 2015. Spearman’s correlation was used to determine the association between these two variables.
Results A positive ecological association was found between STI screening intensity and geometric mean gonococcal minimum inhibitory concentration for ceftriaxone (rho=0.42, p=0.031) and cefixime (rho=0.42, p=0.029), but not for azithromycin (rho=0.31, p=0.11). The above results must be interpreted with caution as many limitations apply.
Conclusions Variation in STI screening intensity may contribute to differences in gonococcal resistance between States in the USA.
- Neisseria gonorrhoeae
- ecological association
- antimicrobial resistance
- screening
- men who have sex with men
Statistics from Altmetric.com
- Neisseria gonorrhoeae
- ecological association
- antimicrobial resistance
- screening
- men who have sex with men
Introduction
In the USA, the Gonococcal Isolate Surveillance Project (GISP) collects gonococcal isolates from men with urethritis presenting at any of its 27 sentinel clinics. The project has found heterogeneity in the prevalence of antimicrobial resistant gonococci between States. This prevalence was highest in some States in the West and lowest in the South.1 The reasons underpinning these geographic variations are incompletely understood.
One explanation is that resistant gonococci, originating from eastern Asia, were introduced into Western States first and then spread eastward.2 A genomic study provided some support for this theory.3 A literature review, however, did not find a consistent association between international travel and gonococcal resistance.4
Alternatively, regional differences in selective antimicrobial pressure may be responsible for the observed geographic pattern. Antimicrobial resistance in Neisseria gonorrhoeae has been linked to recent antimicrobial use at the individual level.5 6 At a population level, gonococcal antimicrobial susceptibility positively correlated with population antimicrobial consumption in a global analysis7 and in a study in 24 European countries.8 Similarly, an analysis from the USA found a link between seasonal variation in macrolide consumption and gonococcal azithromycin minimum inhibitory concentration (MIC).9 An ecological study in the USA with data from 2005 to 2013 did not, however, find an association between antimicrobial use in the general population and gonococcal antimicrobial resistance.2 Nevertheless, ecological studies based on population-level antimicrobial use might underestimate the effect of disproportionately high antimicrobial exposure within subgroups with a high prevalence of gonorrhoea.
The prevalence of resistant gonococci is frequently, but not always, found to be higher in core groups such as men who have sex with men (MSM).1 One possible explanation is that guidelines typically recommend intensive screening for sexually transmitted infections (STIs) in these groups.10 Most gonococcal and chlamydia infections in MSM are asymptomatic and thus screening leads to large increases in antimicrobial consumption, which may in turn select for antimicrobial resistance in N. gonorrhoeae.11 A previous study tested this hypothesis and found an ecological association between STI screening intensity and raised gonococcal MICs for azithromycin and cefixime in 12 cities in the USA.12 In the current paper, we aim to explore the association between STI screening intensity and gonococcal MIC in the USA, based on data from a nationwide behavioural questionnaire and lagged data on antimicrobial susceptibility from GISP.
Methods
STI screening intensity
STI screening intensity data were taken from the American Men’s Internet Survey conducted in the USA from 6 October 2014 until 29 March 2015 (AMIS-2014). This internet-based national cross-sectional survey aimed to collect information regarding sexual and health-promoting behaviour among MSM residing in the USA, aged 15 years or older. Respondents were assigned to a certain State based on their ZIP-code. The full survey methodology is described elsewhere.13 STI screening intensity was calculated as the proportion of respondents per State who indicated that they had been tested for or diagnosed with syphilis, gonorrhoea or chlamydia in the past 12 months.
Antimicrobial susceptibility
Data for gonococcal antimicrobial susceptibility in the USA in 2015 were taken from GISP.14 These data were based on the first 25–30 urethral gonococcal culture isolates from each of the 27 GISP sentinel clinics in 21 different States, taken from male patients regardless of symptom status. The proportion of samples from MSM per clinic was also documented.15 Azithromycin, ceftriaxone and cefixime were chosen as the antimicrobials of interest as these were the most commonly used for the treatment of gonorrhoea and chlamydia since 2007.16 The geometric mean MIC was calculated as the nth root of the product of n MIC values for each antimicrobial.
Statistical analysis
Data were presented as median (IQR). Spearman’s correlation was used to determine the relationship between the geometric mean MIC for azithromycin, cefixime and ceftriaxone per clinic in 2015 as the response variable and (i) the percentage of isolates coming from MSM in GISP-2015 and (ii) STI screening intensity in the corresponding States from AMIS-2014 as the explanatory variables. All analyses were conducted in STATA 13.
Results
STI screening intensity
The AMIS-2014 questionnaire was completed by 9159 respondents. Only the responses of the 6103 (66%) participants living in any of the 21 States that match the 27 GISP clinics were used. The number of respondents per State varied between 39 (Hawaii) and 1063 (California) with a median of 202 (IQR 128–349). Their median age was 40 years old (IQR 28–51). Median self-reported STI screening in the past 12 months was 45.7% (IQR 35.8–47.4) (figure 1). The proportion of respondents that was tested for gonorrhoea strongly correlated with the proportion being tested for chlamydia (rho 0.91, p<0.0001) and for syphilis (rho 0.84, p<0.0001) (online supplementary table 1).
Supplemental material

{kind=link}
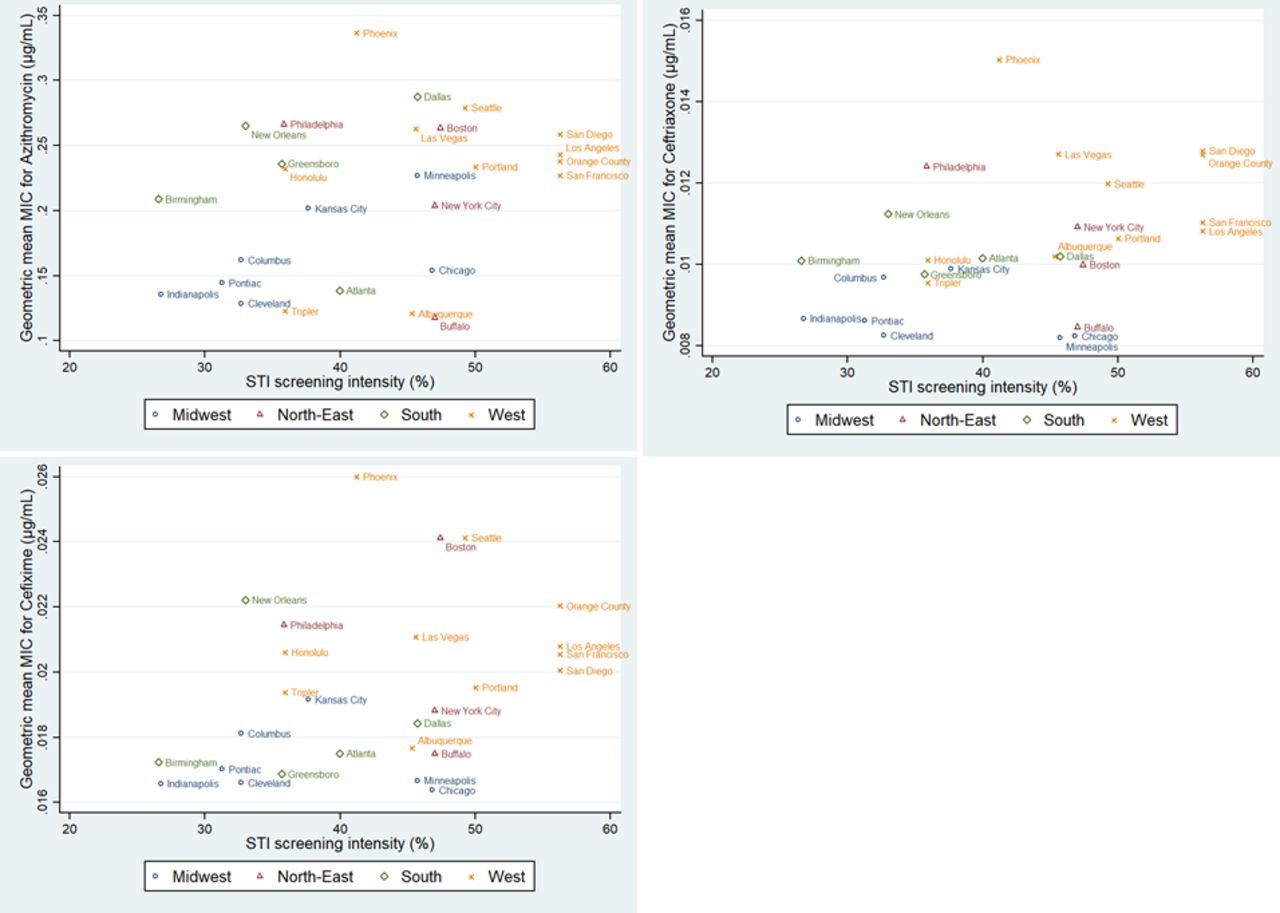
Correlation between geometric mean minimum inhibitory concentration for azithromycin, ceftriaxone and cefixime and STI screening intensity among MSM (data from GISP 2015 and AMIS-2014, respectively). AMIS, American Men’s Internet Survey; GISP, Gonococcal Isolate Surveillance Project; MIC, minimum inhibitory concentration; STI, sexually transmitted infections.
Antimicrobial susceptibility
Median geometric mean MIC was 0.227 µg/mL (IQR 0.144–0.263 µg/mL) for azithromycin; 0.0102 µg/mL (IQR 0.00955–0.0112 µg/mL) for ceftriaxone and 0.019 µg/mL (IQR 0.017–0.021 µg/mL) for cefixime (figure 1).
The proportion of isolates from MSM in 2015 varied between 6.9% (Birmingham, Alabama) and 81.4% (San Diego, California) with a median of 32.5% (IQR 21.9–64.6).14 The proportion of isolates from MSM per clinic correlated positively with geometric mean MIC in GISP for all three antimicrobials (rho 0.42 for azithromycin (p=0.0305), 0.45 for ceftriaxone (p=0.0198), 0.54 for cefixime (p=0.0040)).
Association between STI screening intensity and antimicrobial susceptibility
Reported screening intensity in AMIS-2014 was positively associated with observed geometric mean MIC in GISP-2015 for ceftriaxone (rho=0.42, p=0.031) and for cefixime (rho=0.42, p=0.029) but not for azithromycin (rho=0.31, p=0.11) (figure 1).
Discussion
Gonococcal antimicrobial resistance frequently emerges in core groups. In keeping with this, our ecological study found that gonococcal susceptibility to the antimicrobials under evaluation (azithromycin, ceftriaxone and cefixime) was reduced in clinics with higher proportions of samples from MSM. The reasons for this are imperfectly understood. We hypothesised that the intensity of STI screening might play a role.
We found that there was a twofold variation in the proportion of those reporting screening between States and a moderately positive association between STI screening intensity and gonococcal MIC for two of the three evaluated antimicrobials (for ceftriaxone and cefixime but not for azithromycin). This suggests that STI screening among MSM may play a role in the emergence of antimicrobial resistance.
However, this study has many limitations. First, it is prone to the ecological inference fallacy. Second, the AMIS and GISP surveys may not provide prevalence estimates that are representative at the State level. GISP, for example, collected isolates independent of sexual orientation but noted a fivefold variation between sites in the proportion of samples originating from MSM. Consequently, GISP data may not necessarily provide representative estimates for MSM in certain states.
Third, several biases may have occurred: (i) As stated above, AMIS survey data were the result of convenience sampling (selection bias). Individuals who are more concerned about their sexual health may be more likely to participate in the survey resulting in an overestimation of the proportion of those tested for STIs. (ii) AMIS data relied on self-reported testing and social desirability and/or recall bias may have influenced the responses. (iii) The question we used to estimate screening intensity included either having been tested or diagnosed with an STI in the past year. We may thus have overestimated the proportion of respondents that were screened. However, one would not expect biases (i), (ii) or (iii) to operate differently between States. (iv) The presence of post-treatment samples (indication bias) in GISP may have inflated the true MICs in some clinics as they may be the result of treatment failure15 and treatment failure is expected to occur more frequently in regions with reduced antimicrobial susceptibility at baseline. Still, this would not result in a false positive correlation between STI testing and MIC as long as (fear of) resistance per se is not also a driver of testing for STI.
Last, we did not correct for potential confounders like the proportion of samples from MSM, level of risk behaviour, foreign travel, coinfection with other STIs like HIV, consumption of antimicrobials for other purposes and so on. As antimicrobial resistance is more common among MSM in the USA, this may have caused an underestimation of gonococcal MIC in clinics with a lower proportion of samples from MSM and thus a false positive association between screening intensity and MIC.
Enhanced STI screening has been proposed as an important way to reduce the prevalence of gonorrhoea and chlamydia among MSM at high risk of infection.10 It may also reduce HIV-transmission and the risk of disseminated gonococcal infection. Nevertheless, empirical evidence for any of these benefits is scarce17 18 and no account was taken of possible harm in the form of antimicrobial resistance. The benefits of screening should outweigh its harms.19 Therefore, future studies, preferably randomised controlled trials comparing different intensities of STI-screening among MSM at high risk of infection, should focus on both of these outcomes. One such a randomised clinical trial will commence soon in our and other Belgian STI-clinics.
Conclusion
This paper found a positive association between STI screening intensity in MSM and gonococcal antimicrobial susceptibility in States in the USA. It would be useful to see to what extent this finding can be confirmed by empirical data in a randomised controlled trial.
Key messages
Antimicrobial resistance in gonococci is most prevalent in core groups.
Core groups are frequently screened, and thus treated, for asymptomatic sexually transmitted infections (STIs).
This ecological study aimed to explore the correlation between STI screening intensity and gonococcal antimicrobial susceptibility in men who have sex with men in the USA.
A moderate correlation between STI screening intensity and gonococcal geometric mean minimum inhibitory concentration was found for cefixime and ceftriaxone, but not for azithromycin.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Deborah Williamson
Contributors CK conceptualised, drafted and revised the paper. CVD analysed the data, drafted and revised the paper. JL and SSM-B revised the paper. MZ provided the data from AMIS-2014 and revised the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.