Article Text

Statistics from Altmetric.com
HAART is able to suppress HIV replication and restore specific immune responses. We and others1,2 have demonstrated that previously untreatable progressive multifocal leucoencephalopathy (PML) may improve and has very rarely been reported following HAART. However, CD4+ increase is also associated with inflammatory reactions to previously silent infectious agents, as well as aberrant immune phenomena.3
CASE REPORT
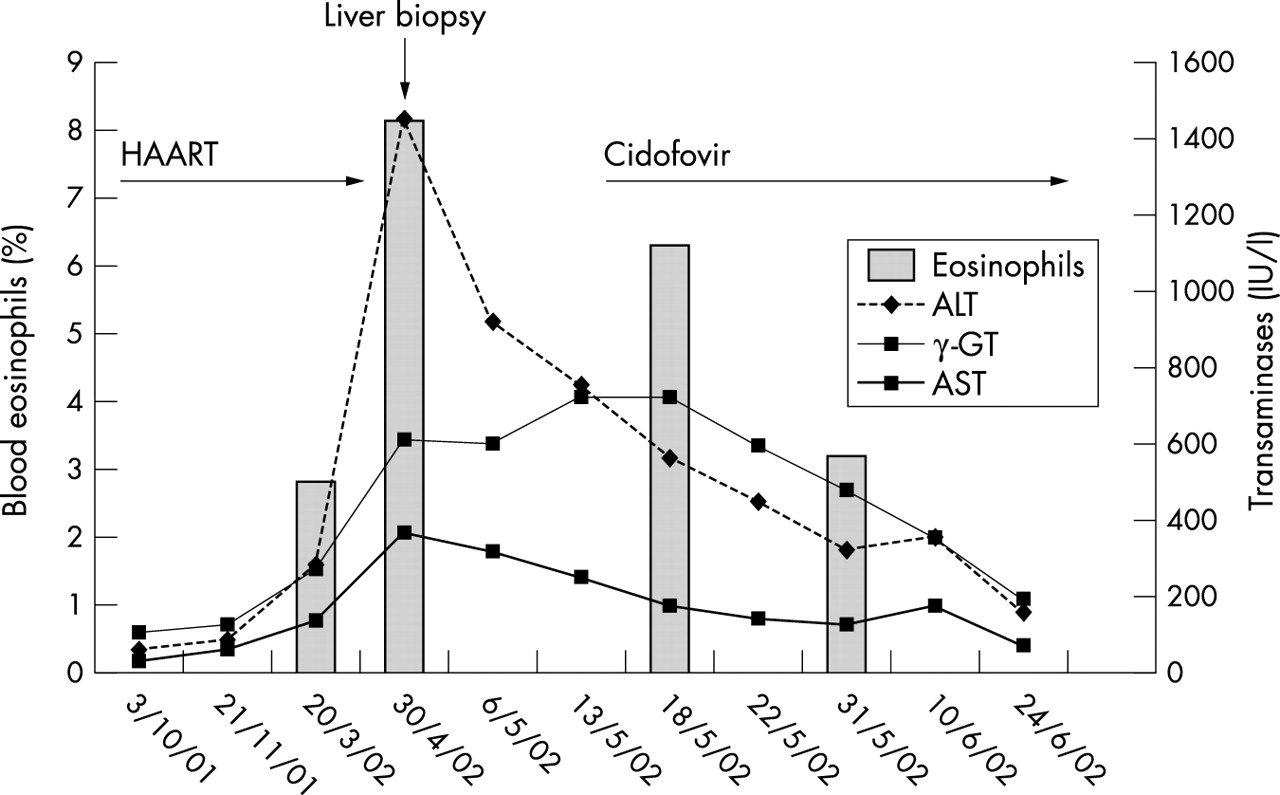
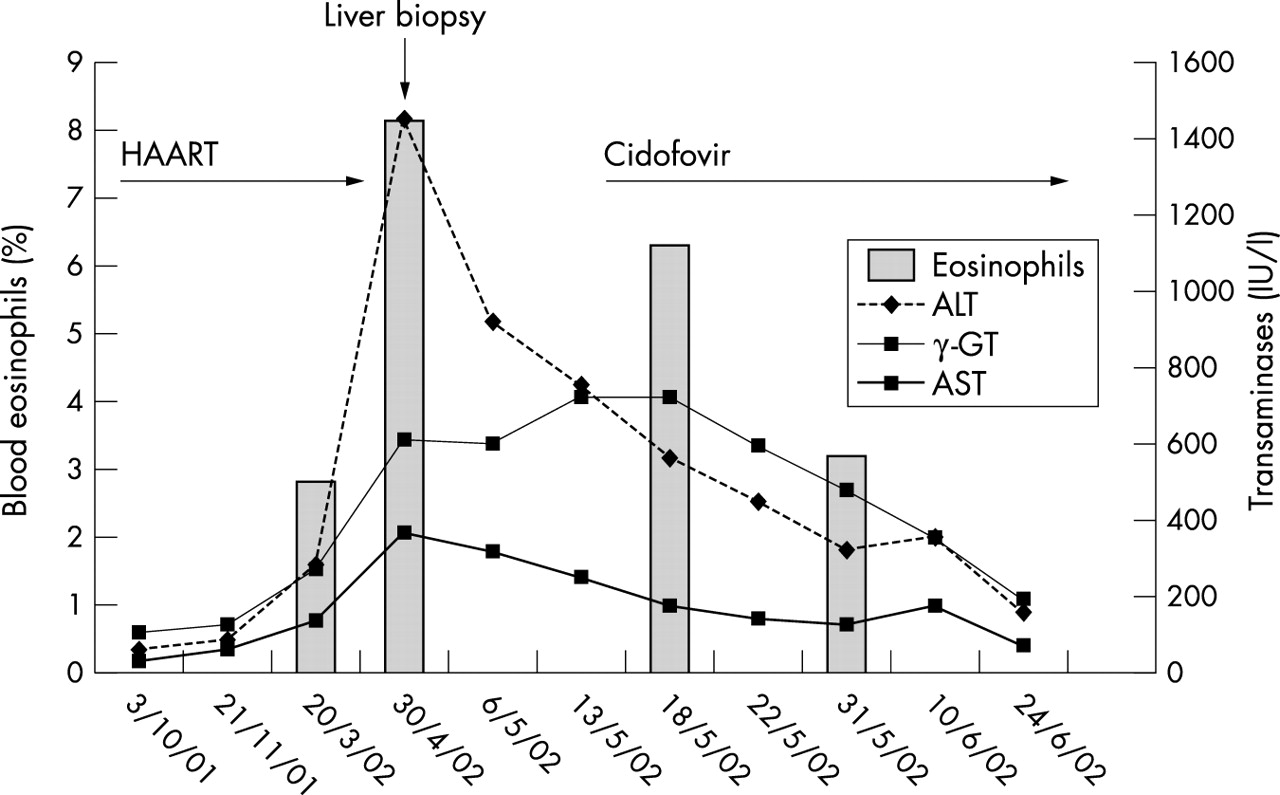
A 27 year old HIV/HCV (hepatitis C virus) patient was observed in 1997 with a CD4+ count of 357 cells ×106/l and HIV-RNA >1 000 000 copies/ml. HAART was started and maintained until 1999 when it was stopped at the patient’s request. On October 2001 he returned asymptomatic, with a CD4+ cell count of 34 ×106/l and HIV-RNA 130 000 copies/ml. Stavudine + lamivudine + nevirapine were then started, together with trimethoprim-sulfamethoxazole. He experienced an optimal response (CD4+ count 159 ×106/l, HIV-RNA <50 copies/ml on March 2002). One month later, the patient was admitted because of mental slowness, aphasia, ataxia, impairment of fine movements of the right arm, and hypostenia of the right leg. He was afebrile and laboratory tests showed WBC 5300 ×106/l, RBC 4550 ×106/l, Hb 16.1 g/dl, PLT: 259 × 109/l, eosinophils 8.3%, AST 369 IU/l, ALT 1446 IU/l, γ-GT 599 IU/l, PT 84%, and raised total plasma IgE 330 IU/ml. Toxoplasma serology, HBsAg, HBsAb, and HAV-IgM were negative; HBc-IgG and HAV-IgG were positive; and HCV-RNA was 172 × 106 copies/ml (baseline 13 ×106/l copies as at October 2001, before HAART). HAART was stopped and liver biopsy performed, showing chronic hepatitis with cholestasis, marked eosinophilia, parenchymal and periportal infiltrates of predominant lymphocytes, and plasma cells suggestive of allergic disease. Cranial magnetic resonance imaging scans revealed subcortical white matter lesions in both frontal lobes and internal capsule with faint peripheral enhancement after gadolinium contrast. Cerebrospinal fluid analysis was normal, fungal and bacterial cultures, cryptococcal antigen, and polymerase chain reaction for HSV-1/2, varicella zoster virus, Epstein-Barr virus, cytomegalovirus, Mycobacterium spp were negative, while JCV-DNA was positive; a cidofovir standard dose was initiated. Subsequently, progressive improvement was observed (fig 1) and PML stabilised.
{kind=link}
Haematochemical clinical course of the study patient.
COMMENT
We report a complex polymorphic immune restoration syndrome of PML (demonstrated also by JCV-PCR in contrast with previous reports2) combined with the first case of liver damage related to delayed immune mediated hypersensitivity reaction to nevirapine.
Several facts support an immunopathogenetic role of aberrant immune recovery in this case: (i) these phenomena occurred together in concomitance with raising CD4+ T cell count under effective HAART; (ii) PML during HAART is exceptional; (iii) both PML during HAART2 and nevirapine hypersensitivity4,5 occurred during the first weeks of therapy in the case series reported so far; (iv) nevirapine hypersensitivity is frequent in conditions of preserved immune response.6 This underlines that pathogenic mechanisms and immunological factors associated with immune restoration diseases may be diverse and unexpected. Moreover, nevirapine hypersensitivity is immediate while this case of liver damage occurred after a substantial period on nevirapine and with concomitant elevation of γ-GT enzyme and increase in HCV replication. Therefore, it would have been very difficult to make the correct differential diagnosis with either late onset metabolic idiosyncrasy to nevirapine or relapsing HCV hepatitis without liver histology. Thus, avoiding liver biopsy in such cases may lead to an underestimation of the causative role of nevirapine.