Article Text

Statistics from Altmetric.com
Although the principal mode of hepatitis C (HCV) transmission in the United Kingdom is injecting drug use (IDU), the risk for a third of infections is unknown.1 The contribution of sexual transmission between men who have sex with men (MSM) to the spread of hepatitis C is unclear, however evidence is accumulating that both co-infection with HIV2 and the presence of other sexually transmitted infections (STIs) facilitate sexual transmission of HCV.3 With the reported increases in unsafe sex and STIs in HIV positive MSM we questioned whether these circumstances may lead to an increase in the number of HCV infections.
This study was undertaken to determine whether within our clinics, changes in the number of individuals being diagnosed with acute HCV infection were occurring and to ascertain risk factors for acquisition in these individuals.
A case note review of all patients within the HIV and sexual health clinics of St Stephen’s Centre with diagnosed acute HCV infection between January 1997 and December 2002 was performed. Patients newly diagnosed with HCV were identified from departmental computer records. Cases were defined as individuals with a newly positive and a previous negative HCV antibody test. Where negative tests had been performed more than a year earlier, testing of stored samples was undertaken to determine more precise timing of HCV seroconversion. Testing was done using the Monolisa anti-HCV version 2 enzyme immunoassay.
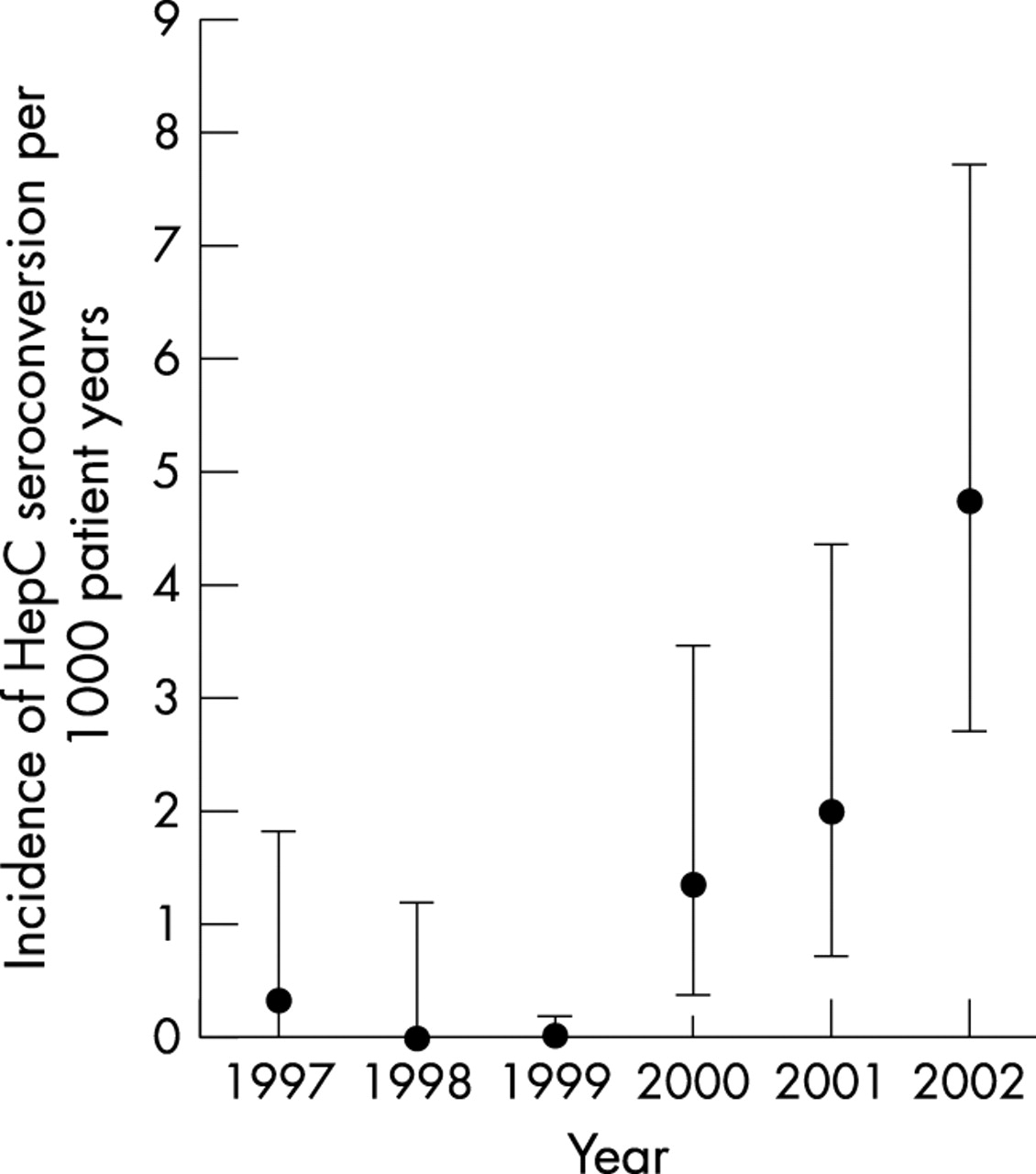
Twenty six male (all MSM) and one female case were identified; median age was 34 years. Twenty five individuals were HIV positive. The median time between negative and positive HCV antibody tests was 5 months (interquartile range 3–10 months). There was a significant increase in HCV seroconversions over the study period (see fig 1).

{kind=link}
Changing incidence of documented HCV seroconversion. Test for trend p value using Poisson regression p<0.001. Error bars are 95% CI. Date of seroconversion was taken as the date of the first positive HCV antibody test.
The indications for HCV testing were the development of abnormal alanine transaminase (ALT) (21), recent IDU (two), sexual contact with HCV positive partner (one), and symptomatic seroconversion (three). Of those tested because of newly abnormal liver function tests (LFTs), 18 were asymptomatic. LFTs were performed as part of routine HIV follow up. There was no increase in HCV tests performed in HIV positive individuals with ALT levels more than 100 IU/l over the study period; however, the percentage of positive HCV tests increased from 0.6 to 9.3 (p value using χ2 test for trend: <0.001).
Risks for acquisition of HCV were recent unprotected anal or vaginal sex (21) and IDU (two), while in four there were no documented risk factors. Nine individuals were diagnosed with infectious syphilis either concurrently (three) or in the year before HCV seroconversion. Of the HIV positive patients 15 were on antiretroviral therapy (ARV) and 11 had a viral load of less than 50 copies/ml. The median CD4 count was 359 cells ×106/l.
Having multiple sexual partners, a history of STIs, and certain sexual practices have been associated with HCV infection. Reported increases in HCV seroconversion among HIV positive MSM in association with high risk sexual behaviour (unprotected anal sex, fisting, and rimming) suggests an interaction between HIV and sexual practice.4 As HCV plasma viraemia is higher in co-infected patients5 and correlates with that in saliva and semen, this may facilitate sexual transmission of HCV. Furthermore, there is evidence that ARV treatment may be associated with increases in HCV RNA levels.6
While retrospective assessment of factors may be problematic, features of this study make us more confident of attributing risk to sexual activity. Data were collected in both general HIV and specialist hepatitis clinics, and also most patients were under long term follow up allowing cumulative recording of risks particularly those relating to IDU.
Although it is possible that increased numbers result from changing HCV testing thresholds there was no evidence of this when we examined HCV tests performed to investigate those with abnormal LFTs, the commonest scenario leading to diagnosis. As the ALT trigger was present in the HIV positive group and not in the sexual health clinic attendees, the numbers from this source may be under-represented.
Determining the associated factors for transmission of HCV is critically important in order to introduce targeted screening and prevention interventions. As 85% of infected patients become chronic carriers and treatment of acute hepatitis C leads to high clearance rates, these strategies may be crucial in reducing the carrier pool of HCV, further transmissions and the risk of cirrhosis and hepatoma.
The study numbers are small and may represent a pocket of infection not indicative of increased risks in larger populations. However, the manner in which these infections parallel recent increases in STIs gives cause for the concern that risks may be more generalised. Further studies are needed to clarify this trend.