Article Text

Statistics from Altmetric.com
Background
In the early summer of 2011, clinicians at Northumberland Sexual Health clinic noticed a sustained increase in cases of gonorrhoea and, more noticeably, a change in case profile from the usual picture of predominantly men who have sex with men (MSM) to heterosexual young adults, with more young females affected. The lead clinician contacted the local Health Protection Team (HPT) to seek advice about investigation and public health interventions. A multiagency outbreak control team (OCT) was convened to coordinate the investigation and control measures.
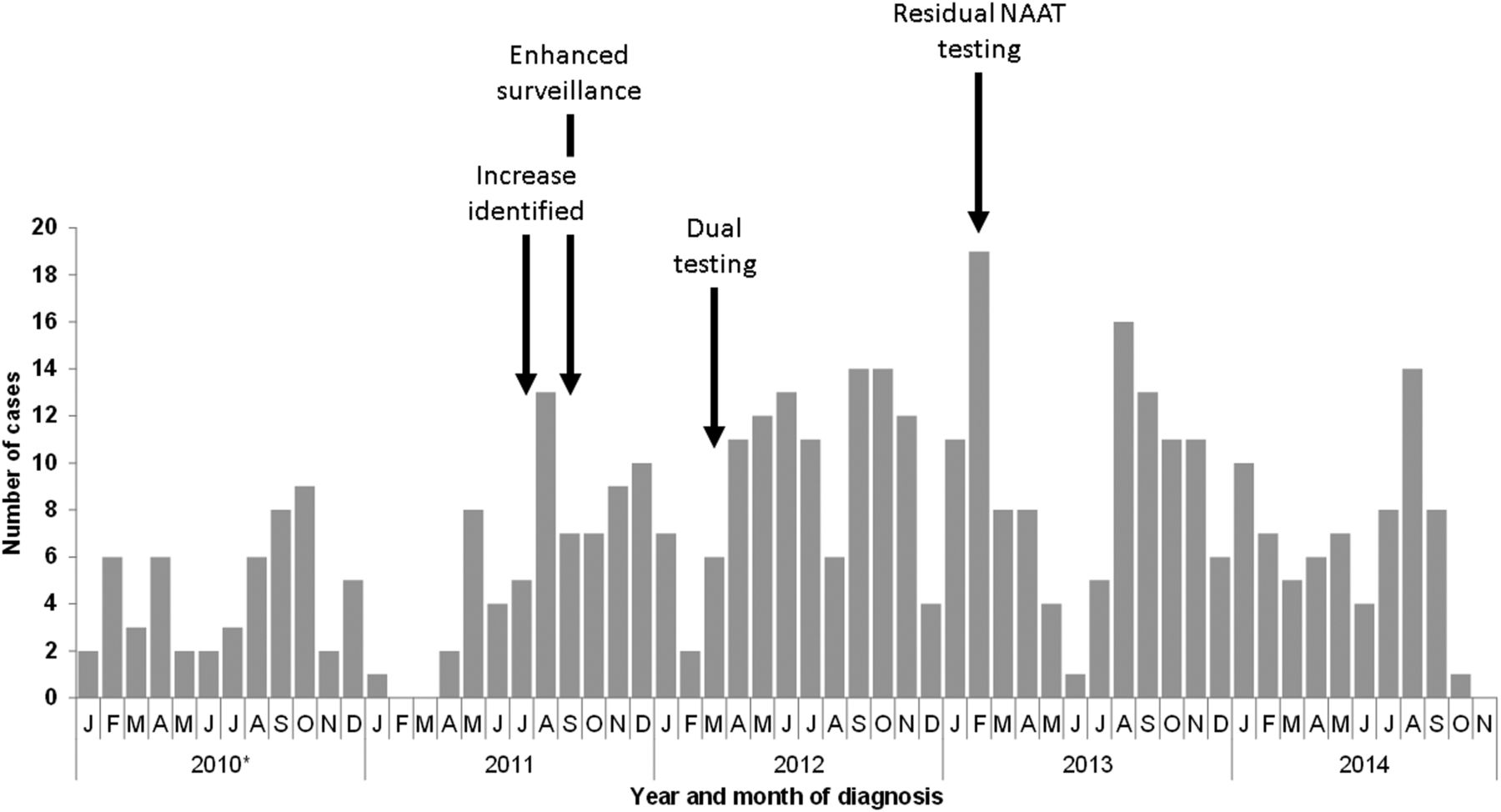
Over the following 3-year period, 360 cases of gonorrhoea were detected in a locally discrete population (figure 1) affecting mainly young heterosexual adults. Patterns of transmission were studied and control measures implemented; however, cases continued to occur at rates higher than pre-outbreak levels.

Epidemic curve of outbreak showing all gonorrhoea cases resident in Northumberland, January 2010 to November 2014, including dates when outbreak control actions were initiated. *2010 data were extracted from GUMCAD, 2011 onwards were from enhanced surveillance.
We describe the approaches taken for investigation and implementation of control measures, reflect on lessons learned and offer advice to colleagues facing similar situations. Figure 1 describes the actions taken over the course of the outbreak investigation.
Clinical management of cases and contacts
Cases were managed according to UK national standards.1 Almost all cases were treated on the day of diagnosis. All patients were advised to return for a test of cure; 50% did and all were negative. Eighty-five per cent of cases were treated with ceftriaxone and azithromycin. All cases were offered a full sexually transmitted infection (STI)/HIV screen; 97% accepted. The main reason for declining a full STI screen was not wishing to have a blood sample collected.
Response to a change in case profile
Guidance on the investigation and management of outbreaks of STIs, including the different teams and organisations that should be included, is available2 and HPTs are well placed to coordinate these activities. HPTs often cover a larger area than the affected service, and as such have an overview of STI epidemiology across wider geography or population groups; they can also access specialist support from national laboratory and epidemiological teams.
The most important part of the process is the early identification of a change in presentation or case profile. In England, routine surveillance of STIs and service use is collated on a quarterly basis but, due to the time taken to collate and disseminate these data, is not designed to detect these types of ‘acute’ changes in STI incidence or to detect discrete local clusters or outbreaks. Therefore, in this situation, the local knowledge and review of cases attending the service were crucial to identifying changes at an early stage.
Recommendations
Sexual health and public health/HPTs should be aware of the local picture of common STIs and have methods for real-time review of case profiles.
Links between clinical and public health teams developed prior to an incident or outbreak through local networks can enable public health interventions to be initiated early and so prevent or alter the course of an outbreak.
Case finding
In this outbreak, the population affected was similar to those targeted by the National Chlamydia Screening Programme (NCSP) that has been operating in England since 2008 (asymptomatic aged 15–24 years).
Six months after the first meeting, the OCT decided to test specimens collected via NCSP for gonorrhoea. A number of factors were considered when making this decision:
The OCT were concerned that as gonorrhoea can be an asymptomatic infection, particularly in women,1 that cases would not present to sexual health services and transmission would continue within the community. Local data supported this, with 60% of female cases and 55% of male cases reporting no symptoms.
Reports from staff involved in the screening programme found that some young people believed that the NCSP sample was tested for ‘all infections’ and that a negative chlamydia result on screening was regarded as a sexual health ‘all clear’.
Local research3 ,4 had highlighted that chlamydia screening was used by young people as a ‘risk mitigation’ approach, that is, the ease of testing and treatment meant that young people preferred to take a test after any unprotected sex than to change their behaviour and use condoms.
The OCT agreed that all these factors could result in infected young people continuing to have unprotected sex and to sustain transmission in the community and so dual testing of NCSP specimens was undertaken.
We had to extend dual testing of NCSP specimens to a wider area than just the ‘outbreak’ because of the catchment area of the NCSP programme; we amended existing NCSP materials to include information about gonorrhoea testing and ensured that information about the additional testing and appropriate referral to sexual health services for treatment was shared with healthcare professionals in primary care and other services. Specific care pathways were developed for the management of cases diagnosed via dual testing as per PHE guidance.5
There was also concern from commissioners about reported high rates of ‘false-positive’ results in a low prevalence area, as had been highlighted in earlier NCSP documents,6 so clear arrangements for review had to be built in to the process.
Results from dual testing identified additional cases which were positive for gonorrhoea-only (35 cases) and therefore would have been missed by the ‘traditional’ chlamydia-only testing by NCSP. Although the gonorrhoea positivity rate from NCSP specimens was 0.4%, lower than for chlamydia (4.7%), almost 17% of all the outbreak cases were identified via NCSP highlighting the benefit of accessing this population with an already accepted and widely used method of testing. The false-positive rate, that is, specimens which were not confirmed on a second assay, for gonorrhoea cases detected through NCSP dual testing was 3% (2 out of 62 cases).
Recommendations
Active case finding, as opposed to simply identifying cases who present to services, is an important activity that can be introduced, particularly if transmission appears to be continuing after control measures have been implemented.
Options for testing through other, pre-existing programmes which target the same audience as outbreak cases should be explored; if these are used, attention should be paid to issues such as consent, patient/client information and pathways into appropriate clinical care.
Defining the extent of the outbreak
Approximately 18 months after the increase in gonorrhoea cases was seen in Northumberland, an increase in cases was reported by clinicians in Newcastle, a neighbouring district. Although the case profile in Newcastle appeared to be predominantly MSM, there were also increases in heterosexual cases. The OCT were keen to determine whether this increase was an extension of the outbreak in Northumberland or part of a more general increase in gonorrhoea, which was being seen across areas of England at that time.7
Following discussion with colleagues from the National Sexually Transmitted Bacteria Reference Unit, it was decided to perform Neisseria gonorrhoeae multiantigen sequence typing (NG-MAST)8 on isolates from outbreak and non-outbreak cases to further understand the epidemiology of cases in the North East.
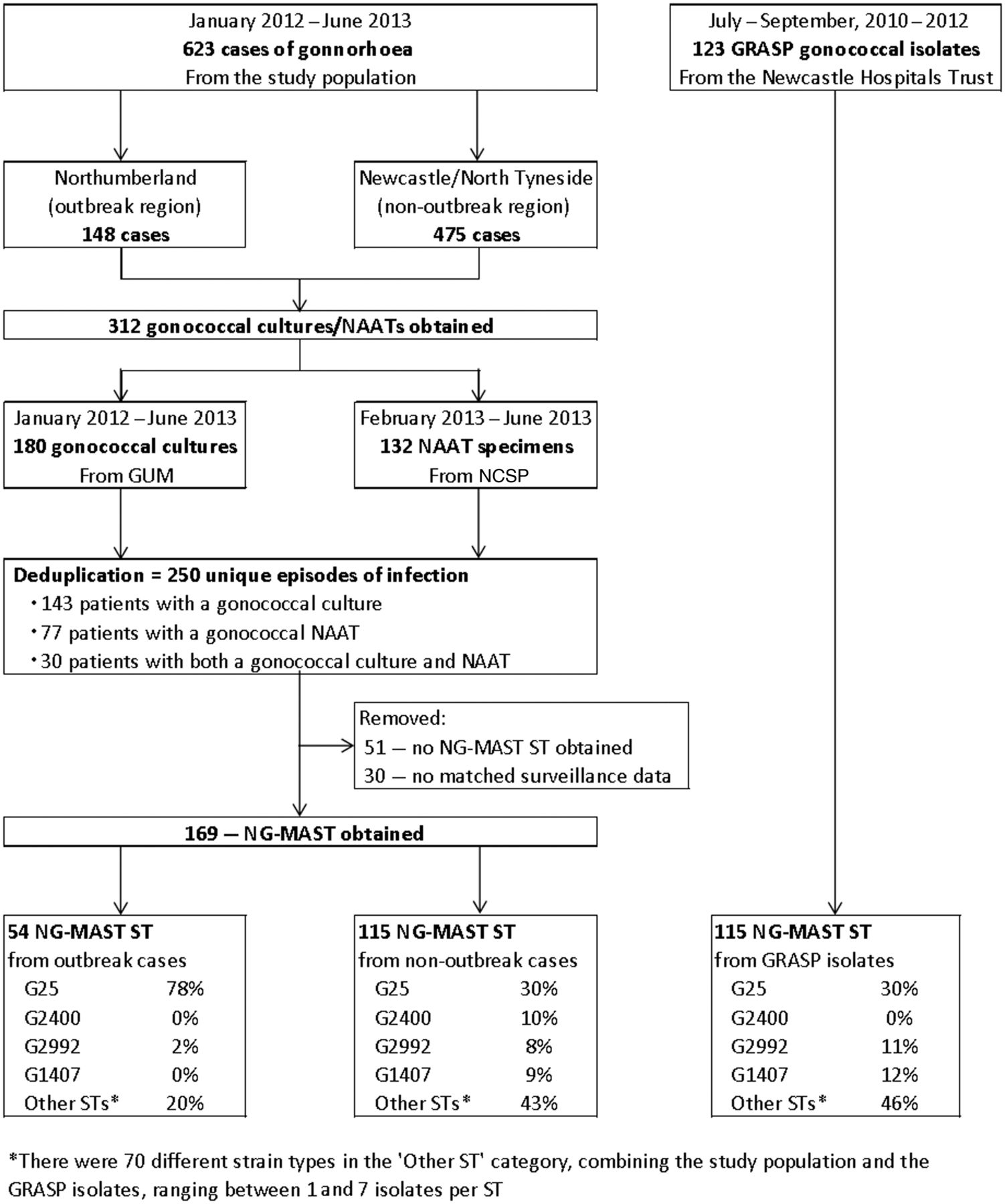
Initially, cultured gonococcal isolates were typed; this was expanded to include residual NCSP specimens to improve the coverage of specimens received (see online supplementary material). The results were also compared with historical regional isolates from the Gonococcal Resistance to Antimicrobials Surveillance Programme (GRASP)9 that were typed to ascertain if the circulating sequence types (STs) were different to recent years (figure 2).
Supplemental material

{kind=link}
{kind=link}
Flowchart showing the specimens collected and Neisseria gonorrhoeae multi-antigen sequence typing (NG-MAST) results for outbreak, non-outbreak and historical isolates. GRASP, Gonococcal Resistance to Antimicrobials Surveillance Programme; NAATS, nucleic acid amplification tests; NCSP, National Chlamydia Screening Programme; STs, sequence types.
The molecular typing identified 49 different STs comprising 22 clusters and 4 genogroups; 25, 1407, 2992 and 2400. The most frequent genogroup was G25 (n=76) which accounted for 45% of all STs. Isolates of G25 were detected in 78% of the typed cases but only in 30% of the typed controls and 30% of the historical GRASP isolates (figure 2).
Using molecular typing of isolates and residual NCSP specimens was a useful adjunct to the outbreak investigation. It added strength to the clinical and epidemiological findings, which suggested that there was a discrete outbreak in Northumberland, as the majority of cases were infected with isolates that were clonal with respect to NG-MAST (G25). The comparison with historical GRASP isolates corroborated this by showing a different profile from background NG-MAST STs in the region.
In this outbreak, only 27% of isolates were typed due to the limited number of specimens cultured (figure 2); the introduction of residual NCSP samples improved the proportions referred and confirmed the reliability of the STs found. The timeliness of the testing and receipt of typing results were dependant on the rapidity of sending the isolates and the availability of laboratory staff as this was additional to routine work.
If we had identified the association between G25 and young heterosexuals earlier in the outbreak, it may have been possible to target partner notification (PN) more effectively, as the molecular typing showed transmission of a NG-MAST ST within this core group.
Recommendations
Molecular typing should be considered to define the extent of an outbreak but there needs to be a plan for specimen selection and collection to ensure good coverage to give meaningful results.
The use of whole genome sequencing in STI outbreaks would offer greater resolution and can provide, in combination with epidemiological investigations, more evidence of transmission events.
Laboratory capacity and resources also need to be assessed along with the timeliness of testing and representativeness and how this could influence control measures.
Enhanced surveillance, PN, contact tracing and describing sexual networks
Initial information about the cases in this outbreak was based on clinical and health advisor records, capturing basic demographic and PN details. Enhanced surveillance was introduced to gather this information in a more systematic way and include more detailed information about ‘exposures’, that is, number of sexual partners, linkages between cases, meetings points/venues, contraception use, history of testing and previous infections.
We also collected enhanced surveillance of gonorrhoea cases from neighbouring sexual health clinics to both identify any cases in neighbouring areas who had exposures in the affected area of Northumberland, that is, people meeting sexual partners in the locality, and to allow us to compare outbreak cases with non-outbreak cases.
Outbreak cases were defined as any gonorrhoea case resident within the Northumberland area (see online supplementary material). We compared outbreak cases with gonorrhoea cases resident in either Newcastle or North Tyneside (neighbouring districts). A multivariable model suggested that outbreak cases were significantly more likely to be white British (p value=0.03), heterosexual (p value=0.05), under 20 years of age (p value=0.07) and have an NG-MAST ST of G25 (p value <0.01).
Staff at the sexual health clinic worked to BASHH standards for PN,10 which recommends 0.6 contacts per index case in clinics outside London. Reaching these targets was particularly challenging in this outbreak. Staff at the clinic made considerable efforts, including home visits to some contacts who were reported as part of extended networks, to identify contacts and ensure attendance for testing, and where necessary treatment. We recognise that the high number of untraceable contacts (31%) means that links between cases, and thus opportunities for intervention, were missed.
Since the outbreak, clinic staff are reviewing approaches to gathering information during the PN consultation, the content of PN messages, methods of communication and engagement of young people in reviewing and designing new approaches (see below).
Sexual networks were mapped to determine whether any localised areas or groups could be targeted (see online supplementary material). Up to the end of 2012, 199 clusters were identified, consisting of a median of three individuals (range 2–22); there were few extended networks (see online supplementary material for technical detail and example of network diagram). As the number of cases increased, network analysis became more labour intensive and could not continue to be completed routinely due to resource limitations.
The enhanced surveillance of these cases was continued until October 2014, when it was agreed by the OCT that the balance of workload for clinical staff versus new information found did not justify the continued collection.
Recommendations
Enhanced surveillance can provide useful additional detail for initial investigation, but care must be taken to review how much new detail is being gained at regular intervals and to balance this against the workload required from clinical and public health teams for its collection and analysis.
A number of template enhanced questionnaires are available and can be easily adapted for local circumstances; the questionnaires should be reviewed and updated as new information or issues come to light to ensure that the process is contributing to refinement of messages or control measures.
Resources for, and approaches to, PN must be kept under close review in these situations; extra effort in the early stages of an outbreak could prevent prolonged transmission within a community.
Awareness raising and public health messages
At the start of the outbreak, the OCT undertook standard approaches to awareness raising, providing information to healthcare professionals in primary and secondary care and to non-health services who worked with young people, for example, schools, youth services. Updates were provided during the outbreak, mainly reminding healthcare professionals that the number of cases was still elevated and to refer young people to sexual health services for treatment and follow-up (table 1).
Table of awareness raising activities
The OCT also considered how to raise awareness among young people. Enhanced surveillance had not identified any specific locations or activities that could be targeted, and advice from communications specialists on the OCT was that ‘traditional’ media outlets (printed press or local radio) were unlikely to be effective in reaching the target audience. Therefore, the OCT agreed to use social media (Facebook) to target information based on age and postcode of users, with pop-up adverts explaining the rise in gonorrhoea, advice on testing and providing links to local sexual health services (see online supplementary materials). Facebook was selected as the preferred platform as it has been used for previous work on chlamydia screening and had received positive feedback from young people; it was also the most popular social media platform used by young people at the time.
Unfortunately, we did not collect robust information about how successful social media advertising was in increasing the uptake of testing. Anecdotal reports from the health advisor team suggested that most young people were attending either because of an affected partner or through general word-of-mouth in the local community.
Recommendations
It is important to consider the different messages and audiences that need to receive information. Involving communication experts in the planning of messages, particularly those to the public, is advised.
Understanding the changing use of social media, where possible consulting young people (through existing focus groups/outreach projects or through specially arranged discussions) to inform communications, is important.
Methods to evaluate, in a real-time fashion, should be built in to the approach; collecting information from service users about the impact of public health messages and adapting messages or approaches as required is advised.
Closing the outbreak
The OCT was disbanded in October 2014; cases numbers had remained elevated, but stable and the group considered that gonorrhoea was probably endemic within the population. Responsibility for the oversight of gonorrhoea in the community was passed to the local sexual health network, which considered population sexual health needs and service provision across all infections.
Reflecting on the outbreak management, we reviewed our performance against available guidance.2 The outbreak management processes were clearly followed but evaluation, both of some of the interventions (see previous sections) and the overall impact of control measures could have been better executed. It was difficult to identify outcome measures that were easily collected through routine data collection; defining the target population and the reach of interventions such as dual testing were not possible as they both covered wider populations; determining how much of any change to chlamydia screening coverage was due to the outbreak interventions was not possible, as there were a number of other initiatives and promotions taking place over the outbreak period which could also have affected these data. We did review the number of young people attending the sexual health clinic for STI testing, but the numbers actually decreased; this may reflect more young people taking up testing via NCSP (unpublished data accessed from the GUMCADv2 database on 17 December 2015).
Recommendation
OCTs should consider process and outcome measures that could be used at the early stages of investigation and, where possible, use routinely collected data.
Discussion
This outbreak highlights a number of issues that all working in sexual health will recognise including how to influence sexual behaviours in young people, identifying and testing sexual contacts and reducing or eliminating transmission in the community.
In the population affected by this outbreak, we were unable to change the behaviours of young people, so relied on prompt testing and treatment of affected cases; however, this was ineffective in reducing transmission due to the continuation of at-risk sexual behaviours.
Qualitative work undertaken with young people in the North East to understand their behaviours regarding sexual health1 ,2 has found some challenges; they regard STIs as being easily treatable, so are less concerned about practising safe sex or using condoms and have a lack of awareness about antibiotic resistance for gonorrhoea. The convenience of testing through NCSP and rapid availability of antibiotics are also seen as a way of managing the risk of unprotected sex, without necessarily leading to behaviour change.
On reflection, we could have tried to engage more young people in the consultation process, specifically those from teenage pregnancy hotspots, but we were restricted by both the need to do things quickly in response to the emerging outbreak and the capacity to undertake meaningful consultation. It may also be useful to develop more proactive and systematic methods to collate and use anecdotal feedback from workers to gain a real-time insight into young people's perceptions about testing and how this may impact on their perception of risk and subsequent behaviours.
Acknowledgments
We thank all members of the outbreak control team for their hard work over the prolonged period of this outbreak. We also thank Dr Jayanta Sarma and Dr Samuel Moses for the initial testing of samples and the forwarding on of specimens, Dr Kirstine Eastick who provide the nested-PCR method, and Nerteley Quaye, Vlad Grigorjev and Marisa Laranjeira for performing the laboratory work. Many thanks to Stephanie Chisholm for her contributions to the study.
Footnotes
Contributors All authors were members of the outbreak control team; all authors contributed to early discussions about the format of the paper. KF drafted the first version and all authors contributed to further versions and agreed final content. AW undertook the analysis of enhanced surveillance data and compiled the network diagrams and MC completed the molecular analysis.
Competing interests None declared.
Ethics approval All work reported was carried out as part of an outbreak investigation and therefore ethics approval was not required. PHE has authority to collect patient-level data for public health monitoring and infection control under section 251 of the NHS Act 2006. Prior to 2013 permission was granted to the Health Protection Agency, PHE's predecessor organisation, under section 251 by the Ethics and Confidentiality Committee of the National information Governance Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data held at Public Health England North East; available to appropriate practitioners for internal surveillance purposes only.