Article Text

Statistics from Altmetric.com
Promising results from the first year of screening
In 2003, the House of Commons Health Committee report on sexual health1 provided a stark and honest insight into the deterioration of sexual health services in England. Contained within a range of hard hitting recommendations aimed at improving sexual health services were a number of recommendations directly relevant to chlamydia prevention and control. These included discontinuing the use of lower sensitivity enzyme immunoassay tests for the diagnosis and confirmation of genital chlamydia in favour of the more sensitive nucleic acid amplification tests (NAATs) and the speedy implementation of a national chlamydia screening programme. Since the publication of this report, additional funding to convert all NHS chlamydia diagnostic tests to NAAT technology has been identified and its implementation is in progress. In this issue four major papers2–5 are presented which inform the development and implementation of the NCSP; we assess their findings and discuss some of the early challenges in implementing this ambitious programme.6
HOW DID WE GET HERE?
Genital chlamydia is now the most common sexually transmitted infection diagnosed in GUM clinics in England, with high prevalence being documented among young men and women aged under 25 attending a variety of specialist and general healthcare settings.7,8 The case for screening for genital chlamydia is now well established, and underpins the implementation of screening and testing initiatives in the United States and a few European countries. Despite uncertainty regarding the natural history of infection—the high disease incidence and prevalence; largely asymptomatic nature of disease; complications and costs of untreated infection; availability of effective simple and relatively cheap diagnostic tests; effective and convenient therapy; and growing empirical and modelling evidence regarding the long term effectiveness of screening programmes9,10 have all been used to call for the implementation of a national screening programme in England.11
In England, the case for screening began in earnest in 1998 with the publication of the Chief Medical Officer’s (CMO) Expert Advisory Committee report12 on Chlamydia trachomatis infection which outlined the public health importance of this disease and the need to screen high risk individuals.
In direct response to the CMO’s report, the Department of Health (DoH), England, funded a variety of demonstration projects aimed at providing additional evidence to inform the development and implementation of a national chlamydia screening programme. Pilots of opportunistic chlamydia screening were undertaken in Portsmouth and Wirral,13 and confirmed the high disease prevalence among those attending healthcare settings, and the feasibility and acceptability of such screening approaches.14,15 Chlamydia testing, funded as part of the National Survey of Sexual Attitudes and Lifestyles (Natsal 2000),16 confirmed the prevalence of disease in the general population and the demographic and behavioural factors associated with prevalent undiagnosed infection. In this issue of STI (p 342), a description of and early findings from the recently completed Chlamydia Screening Studies (ClaSS) in Bristol are presented. This study examined alternative approaches to screening using postal specimens, potential partner notification approaches, and appropriate test/specimen combinations for use in the field. Another DoH funded study examining chlamydia incidence and re-infection among screened individuals is currently under way, with results expected by end 2004. Taken in concert, these studies provide a robust evidence base to inform the initial and subsequent development of the national screening programme.
Concrete plans for a national chlamydia screening programme gained momentum with the publication of the English National Strategy for HIV and Sexual Health,17 in July 2001, which clearly outlined the government’s commitment to a national roll-out of chlamydia screening. This was further strengthened by the publication of an implementation plan in June 2002,18 which confirmed the immediate implementation of screening in 10 areas in England. By September 2002, a national Chlamydia Screening Steering Group (CSSG) with multidisciplinary representation was appointed to advise the DoH on the programme’s design and implementation.
The vision is to implement (by 2008) a multifaceted, evidence based, and cost effective national prevention and control programme for genital chlamydia in England, in which all sexually active adults are aware of genital chlamydia and its effects, and are able to access a range of prevention and screening services to reduce their risk of infection or onward transmission (see table 1).
National Chlamydia Screening Programme, England. Screening populations and locations
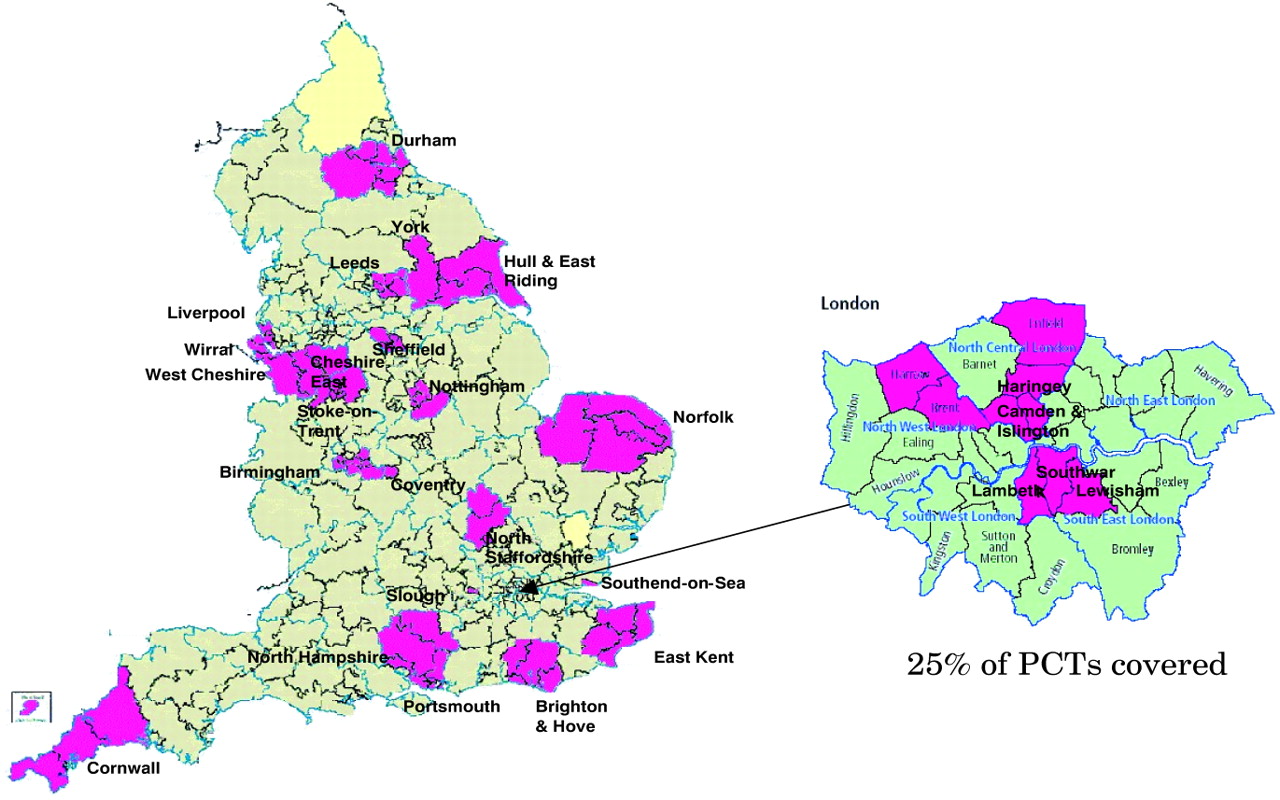
The paper by LaMontagne2 describes in greater detail the objectives, phased implementation and management of the programme and results from the first year of screening. As reported in the paper in the first phase (phase 1), chlamydia screening was introduced in 10 programme areas across England, involving over 300 screening sites with a target population of over 250 000 patients per annum. A further 16 areas were added in January 2004 (phase 2) leading to a total coverage of 25% of all primary care trusts (PCTs) in England (fig 1). Additional programme areas are planned for later in 2004 and successive years. The DoH pump primes the implementation of the programme to each locality providing up to £150 000 for the first year, and full funding for years 2 and 3, after which all local programme costs are to be picked up by the PCT(s). The phased introduction of screening reflects DoH as well as local imperatives. One of the papers in this issue5 models the health care costs of this kind of screening programme and estimates the average cost (with partner management) at approximately £15 per screening offer and £38 per case identified. This model however does not address cost-effectiveness, an analysis that would require greater knowledge of outcomes.
{kind=link}
National Chlamydia Screening Programme, England. Phase 1 and 2 programme areas.
WHERE DOES THIS PLACE US?
The results of the first year of screening has clearly confirmed the feasibility of opportunistic screening approaches outside of GUM clinics and confirms the significant disease burden in this population with 10.1% positivity among women and 13.3% among men. These findings are consistent with the pilot studies14,15 and prevalence estimates summarised in the systematic review by Adams.4 The review also provides further evidence to justify focusing chlamydia screening on people attending health care settings, rather than household screening, given the substantially lower prevalence estimates found in the latter. For example, in women under 20 years, Adams et al report overall prevalence estimates of 12.6% in antenatal clinics and 10.7% in youth clinics, compared with 5.0% in population based studies. Similarly, the paper from the ClaSS group3 describes a range of studies to inform screening methods and includes results from a pilot of active screening in which screening packs were sent to participants homes. The overall response rate of 34.3% was disappointing, with an overall prevalence of 2.8%. This study highlights many of the inherent difficulties with using postal specimens, and although unsuitable as a main screening strategy, it may provide a solution for enhancing screening with particular sub-groups.
CHALLENGES
The national chlamydia screening programme is being implemented within the context of an evolving NHS characterised by devolution of decision making to the local level; heterogeneity in accountability structures and prioritisation by PCTs; and performance management by strategic health authorities. Screening in primary care will require developing a local enhanced service in GP contracts; tackling resistance to further increases in GP workload; clarification of funding for screening activity; and considerable investment in training. The results from the first year of screening nevertheless show that the implementation strategies in England can work, and a variety of non-specialist clinical settings can be enlisted to implement screening. Clearly the challenge now will be to increase coverage at all levels: nationally, within screening programme areas, and within clinical sites offering screening to their patients. Microbiology laboratories in screening areas will require additional investment and training to facilitate the use of NAATs, quality assurance and control. In areas where screening monies are being used to invest in NAATs, care is needed to avoid creating two tier services in which routine diagnostic tests are performed using lower sensitivity assays. The multisite nature of local screening activity, with some sites still not computerised, requires overcoming dataflow logistics and centralising data management. Care will be required not to overload GUM clinics with those screened positive for genital chlamydial infection, and new models of care for managing. These patients and their contacts in the community (either at a local chlamydia office or at screening sites) will need to be evaluated. Finally, as and when local programmes become established, performance management and quality assurance arrangements will be required to ensure that chlamydia screening activity is maintained over time.
Finally, these and other studies confirm the high prevalence of asymptomatic genital chlamydial infection in men and the difficulties opportunistic methods have in identifying and testing them. Although the national chlamydia screening programme actively includes men and women in all screening activities, effective strategies need to be developed, evaluated and good practice shared. Greater effort will be needed to ensure that men themselves are aware of chlamydia, its effects and strategies for its prevention and control. In this regard, the programme has the potential to make a substantial contribution to improving men’s sexual health in the coming years.
These factors aside, the chlamydia screening programme as envisioned in England represents a bold and considered move towards controlling this devastating sexually transmitted infection. The phased implementation will allow further refinement of the structure and process of the screening programme over the coming months; however, successful implementation will only be achieved with a sustained commitment to joint working among stakeholders at local and national levels.
Acknowledgments
All members of the Chlamydia Advisory Group contributed to the preparation of this editorial.
Promising results from the first year of screening
REFERENCES
Linked Articles
- Brief Encounters
- Chlamydia